In the Sensitive laboratory and clinical complex, you can undergo complete clinical diagnostics in Yeysk, including even the most difficult tests. So, to diagnose the condition of the adrenal glands, an analysis is performed for metanephrine and normetanephrine in the urine. These two substances are formed during the transitional stage of the destruction of adrenaline and norepinephrine. A high concentration of metanephrines may indicate the development of an adrenal tumor, since these hormones can be produced by malignant tumors.
But at the same time, the level of metanephrine and normetanephrine in the daily norm can tell a lot about the work of not only the adrenal glands, but also other systems in the human body.
general characteristics
Common metanephrines are intermediate products of adrenaline metabolism. There are three types of catecholamines: dopamine, adrenaline (epinephrine) and norepinephrine. After performing their function in the body, catecholamines are converted into inactive forms. Dopamine - into homovanillic acid, norepinephrine - into normetanephrine and vanillylmandelic acid, and adrenaline - into metanephrine and vanillylmandelic acid. Both the hormones themselves and their metabolites are then excreted in the urine. 55% of adrenaline metabolic products are excreted in the urine in the form of metanephrine. The intratumoral process of metabolism of catecholamines to metanephrines occurs independently of catecholamine secretion. The increase in their level is more significant and persistent than that of plasma catecholamines, and represents a reliable criterion for the presence of the smallest pheochromocytoma (>99% sensitivity, >89% specificity). To increase the likelihood of diagnosis, the study is prescribed in conjunction with the determination of adrenaline and norepinephrine in the urine. When assessing the results of the study, it is necessary to take into account that the content of normetanephrines and metanephrines in the urine may increase after heavy physical exercise, after hypoglycemia caused by insulin, after taking thyroxine preparations, with nephropathies, and hepatitis.
Indications for the determination of metanephrine and normetanephrine in the daily norm
An appointment for this diagnosis in Yeisk can be given by a general practitioner, endocrinologist, oncologist, or cardiologist. The basis for the appointment may be a suspicion of pheochromocytoma. This is a cancerous lesion that begins in the adrenal glands and develops in the nervous system. With the development of pheochromocytoma, the body produces a large amount of catecholamine, which is detected in a urine test.
Pheochromocytoma is expressed in symptoms, the combination of which gives reason for the doctor to prescribe the determination of metanephrine and normetanephrine in the daily urine sample:
- high blood pressure;
- elevated temperature;
- headache and dizziness;
- cardiopalmus;
- nausea and feeling of dry mouth;
- increased sweating.
Patient preparation rules
Preparing for the study:
the day before and during urine collection, it is necessary to: • exclude physical activity (sports training) • for 3 days before the study, exclude food and drinks rich in amines (vanilla, chocolate, coffee, cocoa, tea, cola, beer, bananas, avocados, tomatoes, alcohol), and stop smoking• agree with your doctor on the possibility of discontinuing medications: tetracycline antibiotics, reserpine, tranquilizers, adrenergic blockers, MAO inhibitors, sympathomimetics. To ensure the stability of biological material during the collection period, use a preservative (hydrochloric acid solution), which is necessary get it at the department of ML "DILA".
Collection of biological material
• add the resulting amount of preservative to a clean container for collecting urine (
important
- the volume of the container must be sufficient for the expected amount of urine per day) • do the first morning urination in the toilet. • collect all subsequent daily urine, including the morning portion of the next day into a container with a preservative• throughout the entire collection period, store the biological material in a cool, dark place• after the end of urine collection, determine its volume, mix, pour 35-40 ml into the container that contained the preservative and deliver it to the department of medical treatment "DILA" within 1-1.5 hours after collecting the last portion.
Important!
The container with the preservative must be stored at room temperature out of the reach of children. Avoid contact of the preservative with the skin and mucous membranes. The expiration date of the preservative is indicated on the packaging.
You can add this study to your cart on this page
High levels of metanephrine in 24-hour urine
If, during this diagnosis in Yeisk, the level of metanephrine in daily urine is increased, then this may indicate damage to the diencephalon, or neoplasms in the genitourinary system. If the level of this substance is high, the likelihood of having pheochromocytoma is high, and in order to clarify the diagnosis, a test for total metanephrine and normetanephrine is prescribed. If the thresholds of the elements are elevated, the doctor prescribes functional diagnostics, including MRI, and only after that a course of treatment is prescribed.
High levels of the substance may also be associated with diseases of the hypothalamus, as well as with serious pathologies of the cardiovascular system: myocardial infarction, hypertensive crisis and an attack of angina pectoris causes an increase in the level of this substance in the body.
Indications
Analysis of metanephrines in urine has a high diagnostic value. It is quite sensitive - it clearly detects the disease even at small concentrations and is specific - it allows you to make an accurate diagnosis, while testing for catecholamines is not always advisable, since these substances are destroyed very quickly.
The main indications for determining metanephrines in urine are as follows:
- Diagnosis and observation of catecholamine-secreting tumors: neuroblastoma, ganglioneuroma, pheochromocytoma, paraganglioma, etc.;
- Monitoring the effectiveness of the therapy and predicting the patient’s condition during the rehabilitation period after removal/conservative treatment of the tumor;
- Establishing the causes of hypertensive conditions. If arterial hypertension does not respond well to conservative treatment, then it should be assumed that the pathology is associated with the activity of pheochromocytoma;
- Suspicion of a neuroendocrine disease (based on ultrasound or MRI results);
- Screening of patients at risk (hereditary predisposition).
The results of the analysis are prescribed and interpreted by specialists: oncologist, endocrinologist, general practitioner.
Interpretation:
- For diseases associated with pain, poor sleep, anxiety; during hypertensive crises, during the acute period of myocardial infarction, during attacks of angina pectoris; for hepatitis and cirrhosis of the liver; exacerbation of peptic ulcer of the stomach and duodenum; during attacks of bronchial asthma; after administration of insulin, ACTH; during flights for pilots and passengers. With pheochromocytoma. In sympathetic crises caused by damage to the diencephalic region.
- When the filtration capacity of the kidneys decreases; collagenosis; acute leukemia, especially in children, due to degeneration of chromaffin tissue.
Sample result (PDF)
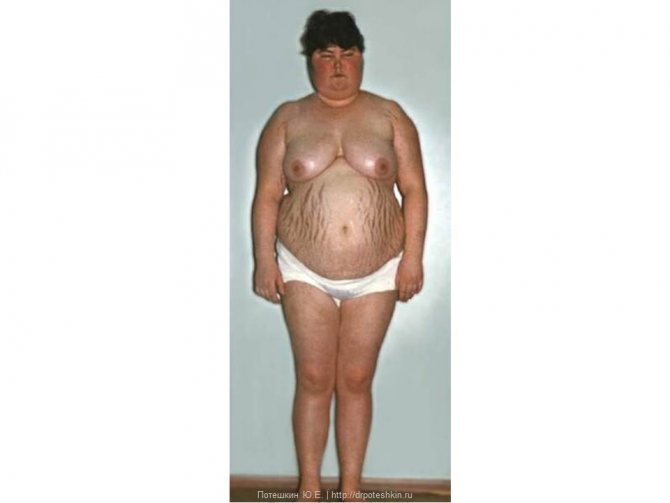
Hypercortisolism syndrome
Clinical picture
- Abdominal fat distribution
- Blush on the cheeks

Acantosis nigricans

Menopausal hump

Other signs
- Striae
- Mycosis
- Hirsutism
- Hypertension
- Psychosis
Metanephrine free in urine (HPLC/MS)
Measurement of 24-hour urinary excretion of metanephrines
is a sensitive screening test that is prescribed for suspected pheochromocytoma.
Blood catecholamines have a short lifespan. Metanephrines
are intermediate metabolites of catecholamines formed from adrenaline and norepinephrine. Measurement of 24-hour urinary excretion of metanephrines is a sensitive screening test for suspected pheochromocytoma. Simultaneous study of fractions of catecholamines, metanephrines and final metabolites of catecholamines (vanillylmandelic-VMC and homovanillic-HMC acids) in urine increases the specificity of the study, reducing the likelihood of false-positive results.
Indications:
- diagnosis and monitoring of catecholamine-secreting tumors - pheochromocytomas, paragangliomas, neuroblastomas;
- differential diagnosis of hypertensive conditions.
Preparation
In the morning, empty your bladder (this portion of urine is poured into the toilet). Record the time of urination, for example: “8:00”. For the next 24 hours, collect all urine excreted in a dry, clean 3-liter jar. The container with urine must be stored in a cool place (optimally in the refrigerator on the bottom shelf at a temperature of 4–8°C), preventing it from freezing.
After urine collection is completed, the contents of the container must be accurately measured. The container must indicate the daily volume of urine (diuresis) in milliliters. For example: “Diuresis: 2000 ml.”
Be sure to mix the urine thoroughly and immediately pour 50–60 ml into a sterile container with a lid. There is no need to bring all the urine collected during the day.
During the entire collection period and until shipment, the biomaterial should be stored in a refrigerator at 2–8°C. The material must be delivered to the medical office on the day the collection ends.
48 hours before urine collection, exclude bananas, pineapples, tomatoes, eggs, chocolate, cheese, as well as foods containing vanillin (confectionery) from the diet. It is necessary to limit as much as possible the intake of products containing caffeine and other stimulants (tea, coffee, cocoa, Coca-Cola). If possible, avoid taking medications 1–2 days before the study, except those used for health reasons.
Interpretation of results
Metanephrine - mcg/day. Alternative units are nmol/day. Conversion factor - mcg/day x 5.07 => nmol/day.
Reference values:
Age-metanephrine-mcg/day:
- children (up to 90 days) - 5.9–37 mcg/day;
- children (90 days - 180 days) - 6.1–42 mcg/day;
- children (180 days - 270 days) - 12–41 mcg/day;
- children (270 days - 1 year) - 8.5–101 mcg/day;
- children (1 year – 2 years) – 6.7–52 mcg/day;
- children (2–6 years old) – 11–99 mcg/day;
- children (6 – 10 years old) – 54–138 mcg/day;
- children (10–16 years old) – 39–243 mcg/day
- adults 0–320 mcg/day
Increasing values:
- catecholamine-secreting tumors of neurochromaffin tissue: pheochromocytoma, paraganglioma, neuroblastoma;
- drug interference: hydrazine derivatives, MAO inhibitors, tricyclic antidepressants, levodopa, bushpirone, significant physical stress.
Description
Free metanephrine and free normetanephrine in the urine are one of the breakdown products of adrenaline.
Used in the diagnosis of adrenal tumors - pheochromocytoma. When is the study scheduled? If pheochromocytoma is suspected. It can be assumed by the following symptoms: persistent increase in blood pressure (and/or episodes of its sharp increase), increased heart rate, hot flashes, sweating. For arterial hypertension that is difficult to treat. If an adrenal tumor or other neuroendocrine tumor was accidentally detected during an ultrasound or MRI examination, or such a tumor was found in the patient’s closest relatives. Research method High performance liquid chromatography-mass spectrometry (HPLC-MS). Units of measurement: mcg/day. (micrograms per day). What biomaterial can be used for research? Daily urine. How to properly prepare for research? Eliminate bananas, avocados, cheese, coffee, tea, cocoa, and beer from your diet 48 hours before the test. Stop taking tetracycline antibiotics, quinidine, reserpine, tranquilizers, adrenergic blockers, MAO inhibitors for 4 days before the study (in consultation with your doctor). Do not smoke for 3 hours before the test. What can influence the result? The level of metanephrine can increase: intense physical activity, coffee, tea, caffeine, alcohol, nicotine, adelphan, insulin, diuretics, paracetamol, propafenone, the antibiotic tetracycline, tricyclic antidepressants, vasoconstrictor drops and nasal sprays, aminophylline. Addresses of offices where you can get tested
Primary hyperaldosteronism
Clinical picture
- Severe hypertension >160–179/100–109 mm Hg.
- Hypokalemia
Diagnosis confirmation - blood test
- Renin
- Aldosterone
Preparing for blood collection
- Discontinue 4 weeks before: Spironolactone, eplerenone, triamterene, amiloride
- Diuretics
- Licorice Root Products
- Verapamil
- When staying in an upright position for no more than 2 hours
Taking blood
- It's best to use a syringe
- Don't clench your fist
- Draw blood no earlier than 5 seconds after removing the tourniquet
- Keep the test tube at room temperature
- Plasma separation no later than 30 minutes after blood collection
- Rapidly freeze plasma
- Stasis - repeated sampling
- Hemolysis - repeated sampling
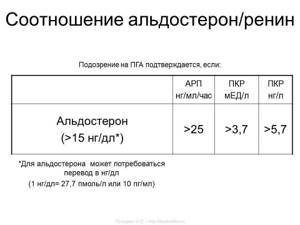
| ARP ng/ml/hour | RCC honey/l | RCC ng/l | |
| Aldosterone (>15 ng/dl*) | >25 | >3,7 | >5,7 |
*Aldosterone may require conversion to ng/dL (1 ng/dL = 27.7 pmol/L or 10 pg/ml)
Saline test
- The most informative test
- For an hour before the test, lie down
- Before the introduction of saline, control - renin, aldosterone, cortisol, potassium
- From 8:00 to 9:30, start infusion of 2 liters of 0.9% NaCl solution
- Carry out the infusion for 4 hours, at the end of the administration the control is renin, aldosterone, cortisol, potassium
Contraindications
- Severe hypertension uncontrolled by drugs
- chronic renal failure
- Decompensated heart failure
- Arrhythmia
- Severe hypokalemia
Interpretation
- PHA is unlikely if aldosterone is less than 5 ng/dL
- PGA is highly reliable if aldosterone is more than 10 ng/dL
- "Gray zone" 5-10 ng/dl
Metanephrines in urine are increased
- Tumors of neurochromaffin tissue (paraganglioma, neuroblastoma, pheochromocytoma, symtoganglioblastoma, etc.);
- Significant stress (physical and emotional);
- Angina attacks, heart failure, myocardial infarction;
- Hepatitis (inflammatory and infectious processes in the liver) and cirrhosis (changes in the size and structure of the liver);
- Hypertension in the acute phase;
- Peptic ulcer during exacerbation;
- Hypothalamic syndrome (impaired control of the sympathoadrenal system);
- Severe nicotine and/or alcohol addiction;
- Treatment with drugs: MAO inhibitors, bushpirone, insulin, hydrazine derivatives, antidepressants, levodopa, etc.