Causes of hematuria
Blood can enter the urine at any stage of urine formation and excretion, so hematuria can be a sign of damage to any organ of the urinary system - kidneys, ureters, bladder or urethra.
An indication of where the problem is located can be determined by the amount of blood present in the urine. If blood is detected at the beginning of urination (in the first portion of urine), then the source of the bleeding is most likely in the urethra. If blood is present in the last portion (detected already at the end of urination), then the source of bleeding is most likely located in the neck of the bladder or in the upper part of the urethra or (in men) in the prostate gland. If blood is present throughout the entire act of urination, then we should expect that the source of the blood is higher - in the kidneys, ureters or bladder. The main causes of blood in urine are:
- infectious diseases. Inflammatory processes lead to circulatory disorders. During inflammatory processes in the kidneys and other organs of the urinary system, a small amount of red blood cells (erythrocytes) may appear in the urine. As a rule, in this case we are talking about microhematuria. However, in women, one of the most common causes of blood in the urine is cystitis, one of the varieties of which - hemorrhagic cystitis - is characterized by the visible presence of blood in the urine (that is, gross hematuria);
- injuries;
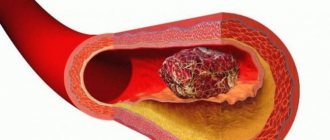
- urolithiasis disease. The resulting stones injure the organs of the urinary system. In some cases, the appearance of blood in the urine is a reason to conduct an examination and identify the disease;
- neoplasms;
- glomerulonephritis. With this disease, the functioning of the renal filtration barrier is disrupted. Normally, it should allow water and relatively small molecules of dissolved substances to pass through, preventing blood cells from entering the urine. Glomerulonephritis causes red blood cells to enter the urine. In this case, microscopy reveals deformation and changes in the color of red blood cells in the urine. This allows us to establish that the cause of blood in the urine is glomerulonephritis.
Pregnant women often experience idiopathic hematuria (ie, hematuria for which the cause cannot be determined). Such hematuria usually stops after childbirth.
Which children are more likely to develop a bladder infection?
Girls are much more likely to develop bladder infections than boys, except in the first year of life. Among boys under 1 year of age, those who have not had their foreskin removed (circumcised) have a higher risk of bladder infection. However, most uncircumcised boys do not develop a bladder infection.
Typically, any medical condition or habit of holding urine in a child's bladder for too long can lead to infection. Other factors that may increase your chance of developing cystitis include:
- overactive bladder, a treatable condition that often goes away as the child gets older;
- incomplete emptying of the bladder;
- waiting too long to urinate;
- constipation—fewer than two bowel movements per week or hard stool that is painful or difficult to pass;
- Vesicoureteral reflux (VUR) is the backflow of some urine from the bladder towards the kidneys during urination;
- A narrowing of the urethra is a problem that restricts the normal flow of urine, such as a stone or a duct that is too narrow (stricture). In some cases, it may be due to a birth defect;
- violations of hygiene rules, defects in caring for a small child;
- family history of cystitis.
Among teenage girls, those who are sexually active are more likely to develop bladder infections. Due to their anatomy, girls are much more likely to develop a bladder infection than boys.
Girls have a shorter urethra than boys, so bacteria have a short distance to travel to reach the bladder and cause an infection.
In girls, the urethra is located closer to the anus, a source of bacteria that can cause a bladder infection.
Classification of the disease in children
- Complicated (with the addition of peritonitis and other ailments) or uncomplicated.
- Acute (accompanied by inflammation of the sub- and mucous layers, in some cases – bleeding of the walls of the bladder) or chronic (morphological pathologies affect the muscle layer).
- Focal or total (according to the degree of prevalence).
- Primary (without abnormalities in the structure and dysfunction of the bladder) or secondary (occurs due to residual urine due to improper anatomy and functionality of the bladder). Source: K.V. Mitrofanov Cystitis in children // Mother and Child in Kuzbass, 2005, No. 1(20), pp. 3-9
Causes of inflammation:
- infection coming from the kidneys, urethra, pelvic and more distant organs;
- dysfunction of the bladder;
- incorrect structure of the organ;
- incomplete and/or irregular bowel movements;
- coli;
- Pseudomonas aeruginosa, Klebsiella, Proteus (rarer pathogens);
- viral infection (indirect effect - leads to improper microcirculation of urine, which becomes a good background for the disease);
- ureaplasma, chlamydia, mycoplasma (usually the cause of infection is chlamydia in parents, as well as lack of hygiene, visiting public baths, etc.);
- phimosis (relevant for boys);
- vesicoureteral reflux;
- fungus (for immunodeficiency).
Additional risk factors for cystitis:
- urolithiasis disease;
- foreign objects entering the bladder;
- therapy with drugs toxic to the kidneys, including cytostatics in oncology;
- invasive examinations on the urological profile;
- dysbacteriosis;
- infection with worms;
- various infectious diseases of the intestinal tract;
- a wide range of gynecological diseases;
- inflammatory and purulent processes;
- dysfunction of the endocrine system;
- radiation;
- hypothermia;
- failure to comply with basic personal hygiene standards; Source: https://www.ncbi.nlm.nih.gov/pubmed/26075187 Hanna-Wakim R, Ghanem ST, El Helou MW, Khafaja SA, Shaker RA, Hassan SA, Saad RK, Hedari CP, Khinkarly RW, Hajar FM, Bakhash M, El Karah D, Akel IS, Rajab MA, Khoury M, Dbaibo GS Epidemiology and characteristics of urinary tract infections in children and adolescents // Front Cell Infect Microbiol. 2015 May 26;5:45. doi: 10.3389/fcimb.2015.00045. eCollection 2015
- etc.
Neonatal sepsis
In newborns, sepsis develops against the background of intrauterine infection. The entrance gate is usually the umbilical wound. Infection may penetrate through the respiratory system, hearing, skin, and gastrointestinal tract. There are fulminant (1-7 days), acute (1-2 months) and protracted (more than two months) sepsis.
Treatment of sepsis in newborns is aimed at suppressing the pathogen, sanitizing purulent foci, and increasing the body's defenses. Antibacterial therapy is carried out taking into account the sensitivity of the pathogen to the antibiotic, and maximum age-specific doses are prescribed for 3–4 weeks. If the sensitivity of the pathogen to antibiotics is not determined, therapy is carried out with broad-spectrum antibiotics. To prevent the development of dysbiosis, probiotics are prescribed.
Also carried out:
- detoxification therapy;
- immunocorrection;
- correction of acid-base balance;
- antishock therapy;
- restoration of water and electrolyte balance.
The prognosis after neonatal sepsis depends on the general condition of the child. The risk of death in premature infants with low body weight is 2-4 times higher. Overall mortality in the early development of sepsis ranges from 3 to 40%. Mortality from late-onset sepsis depends on the etiology of the infection.
Infant

Blood in the urine of infants found in a diaper is a real shock for all parents. However, you should not worry in advance, because the red color of urine does not always indicate the presence of some terrible disease. Here are some reasons for this phenomenon:
- hormonal disorders in girls;
- constipation;
- dermatitis;
- cracks in the mother’s nipples (provided that she is breastfeeding);
- allergy;
- lactose deficiency;
- infections;
- volvulus;
- eating food with red pigment.
Please note that a baby’s blood vessels are very fragile, and almost any health problem can lead to their damage. The cause could even be high temperature or overwork. Causes of hematuria in an infant:
- cystitis, urethritis (which are a consequence of poor hygiene and the development of infections in the urinary tract);
- pathologies;
- glomerulonephritis;
- hemorrhagic diathesis.
Additional diagnostic methods
It is extremely important for parents to provide as complete information as possible about the child’s condition, and to be prepared for a number of additional diagnostic procedures (ultrasound, MRI, examination of the bladder, X-ray studies) and laboratory examinations (24-hour and fractional urine tests, clinical blood tests).
All this will be the key to establishing the correct diagnosis and carrying out therapy as soon as possible.
This article does not constitute medical advice and should not serve as a substitute for consultation with a physician.
Sepsis: clinical guidelines
Sepsis is treated in intensive care units or intensive care units. Sanitation of the source of infection is necessary - for example, opening an abscess, removing pus and dead tissue in the area of inflammation.
Etiotropic therapy is carried out as early as possible. Before identifying the pathogen and determining its sensitivity to antibiotics, broad-spectrum antibacterial drugs are prescribed. If the primary source of infection has not been established, consider whether the infection is community-acquired or hospital-acquired. For community-acquired infections, the drugs of choice are third and fourth generation cephalosporins and fluoroquinolones. For hospital infections, carbapenems are prescribed. Important: the administration of high doses of antibiotics over long courses is required to create the necessary concentration of the drug in the blood and at the sites of infection.
In case of sepsis, clinical recommendations for the treatment of patients with anaerobic infections are the use of metronidazole and lincosamide antibiotics. For staphylococcal sepsis, anti-staphylococcal immunoglobulin is administered. Etiotropic treatment is carried out until the symptoms of infection disappear and stable positive dynamics of the patient’s condition appear.
The primary measures for sepsis include infusion therapy. It helps to correct tissue perfusion and homeostasis, normalize cellular metabolism, and reduce the concentration of toxic metabolites.
In case of emergency conditions arising from sepsis, additional measures may be required:
- artificial ventilation;
- hormone therapy;
- treatment of acute renal failure;
- blood glucose control;
- maintaining cardiac activity;
- prevention of deep vein thrombosis.
Symptoms of sepsis in adults
Sepsis - what is this disease? Pathology is manifested by a violation of the general condition of the body. Secondary foci of infection may also occur.
Symptoms of sepsis in adults:
- headache;
- confusion;
- temperature rise to 39-40 degrees;
- tachycardia;
- decrease in blood pressure;
- swelling;
- progressive weight loss;
- thrombosis.
In severe sepsis and septic shock, there is a disturbance in the blood supply to individual organs and tissues. Septic shock occurs more often in children, the elderly, and people with immunodeficiency. Multiple organ failure in sepsis (it develops when many organs are affected - this is the so-called multiple organ sepsis) ends in death in 25–45% of cases.
The clinical course of the disease can be fulminant (1–2 days), acute (up to 1 week), subacute (more than 1 week), and chronic. With sepsis, symptoms may be blurred or atypical. With the development of sepsis in newborns, vomiting, diarrhea, rapid weight loss are observed, suppuration in the navel area, abscesses and phlegmon of various locations may appear.
Complications of sepsis include: hemodynamic, respiratory, renal, neurological, cardiac disorders. Thrombocytopenia of unknown etiology is observed in 10-30% of patients with sepsis. Read more about the complications of this pathology on our website Dobrobut.com.
Diagnosis of sepsis is based on an analysis of symptoms and laboratory data (isolation of the pathogen and determination of its sensitivity to antibiotics, procalcitonin test, blood and urine tests).