Hysteroscopy of the uterus is both a diagnostic and therapeutic procedure that allows you to examine the uterine cavity from the inside and, if necessary, perform various medical procedures, for example, remove foreign bodies, polyps, etc. Hysteroscopy is performed using special instruments that are inserted through the vagina.
- Types of hysteroscopy of the uterus
- Indications for performing hysteroscopy of the uterus
- How to prepare for hysteroscopy of the uterus
- How is hysteroscopy performed?
- Contraindications
- Recovery after hysteroscopy of the uterus
- What complications can hysteroscopy cause?
- What procedures can a gynecologist perform during hysteroscopy?
- When can hysteroscopy be performed?
- Risks of hysteroscopy
- What alternatives are there to hysteroscopy?
Types of hysteroscopy of the uterus
- Diagnostic hysteroscopy. As the name implies, this procedure does not involve therapeutic interventions. During diagnostic hysteroscopy, only a visual examination of the internal cavity of the uterus and cervical canal is performed using a special optical system. Since no surgery is performed, significant anesthesia is not required. In most cases, local anesthesia and sedation are sufficient. The recovery period after the procedure is short. No hospitalization required.
- Surgical hysteroscopy is already a therapeutic and diagnostic intervention. It allows you to detect the problem and immediately treat it. This procedure is prescribed when the diagnosis has already been established, or in cases where its probability is maximum. This is already a full-fledged operation, albeit a low-traumatic one. It requires anesthesia and is therefore performed in a hospital setting.
- Control hysteroscopy. It is carried out to monitor the condition of the uterus after surgical treatment.
Indications for performing hysteroscopy of the uterus
- Infertility of unknown etiology.
- Habitual miscarriage.
- Polyps of the uterus and cervical canal.
- Foreign bodies in the uterine cavity, for example, intrauterine contraceptives.
- Pathology of the endometrium - hyperplasia, synechiae.
- Suspicion of uterine malformations.
- Metrorrhagia is non-cyclic uterine bleeding.
- Bleeding after menopause.
Currently, there is a trend away from carrying out invasive techniques purely for the purpose of examination, since this is one way or another associated with certain risks, and the necessary information can often be obtained using safer methods. The same applies to diagnostic hysteroscopy. The procedure is prescribed only if it is impossible to establish a diagnosis using other non-invasive methods.
Book a consultation 24 hours a day
+7+7+78
How to prepare for hysteroscopy of the uterus
Hysteroscopy of the uterus is an invasive procedure that carries certain risks. To minimize them, it is necessary to undergo examination and, if indicated, treatment. As part of the examination, the following tests are prescribed:
- General and biochemical analysis of blood and urine.
- Smear for flora and oncocytology (if not performed within the last year).
- Test for STIs.
- Coagulogram.
- Determination of blood group and Rh factor.
- ECG.
- Determination of markers of infectious diseases: HIV, parenteral hepatitis, syphilis.
If inflammatory gynecological processes are detected, sanitation is carried out.
Hysteroscopy is planned in accordance with the menstrual cycle. It is recommended to perform the procedure in the first days after the end of menstruation, since during this period there is no growth of the endometrium and it is easier to detect its pathology. However, if there are absolute medical indications, the procedure can be performed on any day of the cycle. Immediately before hysteroscopy, you must adhere to the following rules:
- Avoid vaginal sex 1-2 days before the scheduled procedure.
- The last meal should be at least 6 hours before the start of the intervention. This condition is necessary for safe anesthesia. Anesthesia can lead to muscle relaxation and the flow of gastric contents into the airways. This is fraught with the development of asphyxia or aspiration pneumonia, which is difficult to treat.
- You will need to shower on the day of surgery.
- Before the operating room, you must empty your bladder and remove jewelry, dentures, and contact lenses.
Care
Let's talk about how to take care of yourself after it.
- Medicines . Anti-inflammatory drugs are prescribed once or in a course of up to 5 days. Doctors are playing it safe and want to prevent the inflammatory process. Gentle antibiotics are prescribed to eliminate any risk of infection.
- Hygiene . For the first 2-3 weeks, it is recommended to wash yourself twice a day, using delicate products. Clean the external genitalia and surrounding skin. When washing, move from top to bottom, from the entrance to the vagina to the anus - this way there is less risk of infection.
- Observation . Monitor your temperature during the first week after the procedure - measure it twice a day (morning, evening). Pay attention to the nature of the discharge - its color, abundance.
Temporarily prohibited
- Warming procedures. Hot bath, solarium, bathhouse and sauna are prohibited for the first 2 weeks. They increase blood circulation and can cause bleeding and inflammation.
- Exercise stress. For the first 14 days, it is contraindicated to play sports and lift weights over 5 kg. Return to physical activity gradually, loading your body moderately.
- Swimming. Pool classes are excluded for 2 weeks. The cervix must recover to fulfill its protective function. Also refrain from water activities on lakes and seas.
- Sexual contacts. Sexual rest for the first 14 days is necessary to avoid inflammation and allow the mucous membrane to recover.
- Vaginal products. Stop using sanitary tampons and vaginal products (suppositories, ointments) for 3 weeks.
How is hysteroscopy performed?
An hour before the patient is admitted to the operating room, premedication is administered, the purpose of which is to reduce anxiety, increase tolerance to anesthesia and reduce the secretory activity of the glands. For this purpose, a combination of drugs is prescribed, containing narcotic analgesics, antihistamines, anticholinergics and sedatives.
In the operating room, the patient is placed in a gynecological chair and anesthesia is administered. The type of anesthesia is discussed in advance, taking into account contraindications, recommendations of the anesthesiologist and the wishes of the patient.
Next, proceed directly to hysteroscopy:
- The cervical canal is expanded using special instruments.
- A sterile liquid or gas is injected into the uterus through an enlarged canal. This is necessary to expand its cavity and make it accessible for inspection and manipulation.
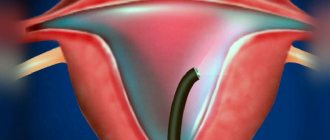
- Next, a hysteroscope is inserted through the cervix - a thin tube with a diameter of about 5 mm with an optical system that transmits an enlarged image to the monitor. As it is introduced, the cervical canal, intrauterine cavity and its angles are examined.
- After the diagnosis has been established, treatment is carried out using the same hysteroscope, which has a special channel for inserting surgical instruments. In this way, removal of polyps, submucosal myomatous nodes, dissection of synechiae, curettage of the endometrium, etc. can be carried out.
- After all interventions are completed, the hysteroscope and the injected liquid or gas are removed. The patient is sent to the intensive care ward, where she recovers from anesthesia under the supervision of medical staff.
Methods for removing endometrial polyps
Surgical removal of endometrial polyps is called polypectomy. It involves curettage of the endometrium followed by histological examination of the resulting material. Curettage can be performed blindly, under visual control using ultrasound or hysteroscopy. The latter method is the most preferable because it allows you to control the completeness of polyp removal and avoid the development of surgical complications (uterine perforation, excessive curettage with damage to the basal layer of the endometrium, etc.).

If treatment does not help, and the patient is in menopause, she may be offered surgery to remove the uterus in the following cases:
- Persistent relapses of multiple polyposis.
- High risk of malignancy of polyps.
- The presence of severe symptoms that significantly worsen a woman’s quality of life.
Recovery after hysteroscopy of the uterus
The recovery period after hysteroscopy is divided into two stages. In the early recovery period, tissues damaged during the procedure are restored—the mucous membrane of the uterus, the muscular wall, and the cervical canal. This period lasts about 2-3 weeks.
The second period takes about six months. At this time, the new endometrium will be regenerated, which must meet the functions assigned to it - grow and be rejected in the process of changing the phase of the menstrual cycle.
Bloody discharge after hysteroscopy
Moderate bleeding is possible in the first 2-3 days after hysteroscopy. This is normal, since during the procedure the cervical canal, endometrium and muscular layer of the uterus are injured. Gradually, the discharge lightens, acquires a yellowish color and continues for about 2-3 weeks. If heavy bleeding develops, you should immediately consult a doctor, as this may be a symptom of serious complications.
Painful sensations after hysteroscopy
Mild to moderate pain after hysteroscopy is normal. They are localized in the lower abdomen and can radiate to the sacrum or lower back. They arise due to stretching of the uterine cavity and injury to the cervix. To alleviate the condition, it is recommended to prescribe “strong” NSAIDs such as ketorol or indomethacin. If the pain increases and becomes unbearable, you should seek medical help immediately, as this may be a sign of serious complications.

In order for the recovery period to go smoothly, you must adhere to several rules:
- Take all medications prescribed by your doctor. As a rule, we are talking about antibiotics that are prescribed prophylactically to prevent the development of infections.
- Avoid vaginal sex until your next period.
- During the period of bleeding, it is better to use pads. Tampons are strictly prohibited.
- Also, during the recovery period it is not recommended to use vaginal suppositories, tablets and creams.
- Refrain from intense physical activity.
- Don't forget about personal hygiene. Toilet of the genital organs should be performed at least 2 times a day, and ideally after each urination and defecation.
- To prevent the development of constipation, follow your diet. Don't forget to empty your bladder in a timely manner.
Uterine curettage and hysteroscopy
Curettage of the uterus is the most common minor operation in gynecology. Among themselves, women often call this operation “cleansing.” But, unfortunately, doctors do not tell all patients about the essence of this operation in an accessible form, but curettage is often a very important step in the treatment of the patient.
Why is uterine curettage performed?
Typically, curettage of the uterus has two purposes - diagnostic (obtaining material - scraping the mucous membrane - for histological examination) and therapeutic (stopping bleeding or removing pathologically altered mucous membrane of the uterus).
Indications for uterine curettage in gynecology:
- Suspicion of endometrial hyperplasia or polyp detected by ultrasound. Endometrial hyperplasia is an excessive growth of the uterine mucosa, when it becomes thicker than it should be normally during a given phase of the menstrual cycle. An endometrial polyp is a pathological tumor-like formation “on a stalk”, growing from the mucous membrane of the uterus.
- Acyclic bleeding and uterine bleeding
- Any bleeding in postmenopausal women
- Suspicion of chronic endometritis (chronic inflammation of the uterine mucosa) as one of the causes of female infertility
- Non-developing (frozen) pregnancy
Are there any contraindications to uterine curettage?
Curettage of the uterus is not routinely performed in case of inflammation in the vagina and cervix (presence of purulent discharge from the genital tract and inflammatory changes in the vaginal smear), as well as the general serious condition of the patient due to advanced age and concomitant diseases of the heart, lungs, liver, kidneys, blood, when the risk of pain relief and the intervention itself is quite high.
How is uterine curettage performed?
Uterine curettage is a minor gynecological operation, which in the vast majority of cases is performed under general anesthesia. Intravenous anesthesia is usually used. After a special drug is injected into a vein, the patient falls asleep and wakes up in her room when the operation is completed. If there are contraindications to intravenous anesthesia or allergies to certain drugs, curettage may be performed under local anesthesia. In this case, an anesthetic drug (novocaine or lidocaine) is injected into the cervix and vaginal vaults. When local anesthesia is used, the patient remains conscious throughout the operation.
The operation of curettage of the uterus is usually performed in the so-called small operating room on a gynecological chair. The average duration of the operation is 10 – 15 minutes. After the onset of anesthesia, the external genitalia and vagina are treated with an antiseptic solution. Then the cervical canal is gradually expanded with special Hegar dilators so that the instrument can be inserted into the uterine cavity. Next, curettage is performed, which means scraping the mucous membrane from all the walls of the cervical canal, and then the uterine cavity. These two scrapings are sent separately for histological examination to distinguish between pathological conditions of the cervix and the endometrium (the lining of the uterus). When curettage of the uterus due to a non-developing (frozen) pregnancy, the uterine cavity is immediately scraped out, using vacuum aspiration (“suction” of the contents of the uterine cavity). At the end of the operation, the vagina is re-treated with an antiseptic solution, and ice is placed on the patient’s stomach for 15 to 20 minutes.
What is hysteroscopy?
Usually, uterine curettage is not just done “blindly”, but is supplemented with hysteroscopy, that is, examination of the uterine cavity using a special “optical tube” - a hysteroscope. Hysteroscopy is performed immediately after dilation of the cervical canal before curettage. During hysteroscopy, the doctor during the operation examines the cervical canal, the uterine cavity, studies the mucous membrane of the uterus, can see various pathological formations in the uterine cavity (polyps, fibroid nodes), and then remove them “targetedly”, under visual control, and not “ “blindly”, as with conventional curettage. Repeated hysteroscopy is performed immediately after curettage in order to examine the walls of the uterine cavity and control the completeness of removal when curettage of all pathologically altered mucous membranes and formations (endometrial polyps).
What complications are possible after uterine curettage?
Curettage of the uterus is the most common, “routine” operation in gynecology, which, although quite rare, can, like any other surgical intervention, be accompanied by certain complications.
Possible complications of uterine curettage:
- Tears or ruptures of the cervix - occur when the cervical canal expands. More often, this complication is observed in nulliparous women and postmenopausal women.
- Uterine perforation is the formation of a through hole in the wall of the uterus. Since curettage is an operation performed “blindly”, based on the doctor’s tactile sensations, such a complication is possible. Often this is facilitated by pathological processes in the uterus itself, when its walls become thinner and loosen, or the entire uterus is deformed and sharply tilted to the side. When the uterus perforates, it is necessary to perform an operation - suturing the uterine wall, and sometimes removing the uterus.
- Inflammation of the uterus and appendages. Since the operation is performed through the vagina, an organ populated by a large number of microorganisms and bacteria, it is impossible to create absolutely sterile conditions during the operation. In some patients, even despite preparation and antibacterial prophylaxis, inflammation of the uterus and uterine appendages occurs. In this case, there is a need for antibacterial and anti-inflammatory therapy.
- Hematometra (accumulation of blood clots in the uterine cavity) most often occurs in nulliparous women, and after curettage of the uterus due to a non-developing pregnancy. This usually involves vacuum aspiration (“suction”) of blood clots and treatment with drugs that contract the uterus (oxytocin).
Almost all complications can be avoided if the operation is performed with grade I–II purity of vaginal smears, antibacterial prophylaxis is used, the operation is performed carefully, and hysteroscopy is used.
What to do after curettage of the uterus?
Usually, after curettage of the uterus, patients are discharged home on the day of surgery or after 1 to 3 days. Within 7–10 days, bloody discharge from the genital tract is possible. Resumption of sexual activity is recommended after the cessation of discharge from the genital tract. Approximately 7 days after the operation, it is necessary to obtain a conclusion from a histological examination of scrapings of the mucous membrane of the cervical canal and the uterine cavity obtained during curettage. Histological examination data are necessary to determine the tactics of further treatment (drug treatment, Mirena medical coil or surgery).
What complications can hysteroscopy cause?
As with any invasive intervention, complications may develop after hysteroscopy. The most formidable and dangerous of them is perforation of the uterine wall, which is accompanied by bleeding. To eliminate the perforation, repeated surgery is required to suturing the defect. If left untreated, peritonitis may develop.
There may also be other complications:
- Hematometra is the accumulation of blood in the uterine cavity due to the impossibility of its drainage. Clinically manifested by increasing spasmodic pain in the lower abdomen and deterioration in general well-being. For treatment, conservative methods can be used (prescription of drugs that improve uterine contraction or antispasmodics for pathological contraction of the cervix), or surgical methods, in which repeated intervention is performed with evacuation of the intrauterine contents.
- Infectious complications. They are manifested by an increase in body temperature, symptoms of intoxication, and pain in the lower abdomen. A little later, pathological discharge appears, which may have a foul odor.
- Bleeding. Possible after therapeutic hysteroscopy, when, for example, myomatous nodes or polyps are removed. If you experience heavy bleeding, especially if it lasts several days, you should consult your doctor.
In general, hysteroscopy is a low-traumatic intervention and the likelihood of complications after it is much lower than with other, more extensive treatment methods.
Signs of a polyp in the uterine cavity and their diagnosis
Often uterine polyps do not manifest themselves, but some patients have the following symptoms:
- Menorrhagia - heavy menstruation.
- Bleeding outside of menstruation.
- Spotting after sexual intercourse.
- Bleeding during menopause.
- Infertility and miscarriages.
- With large polyps, women may notice copious whitish discharge, discomfort and pain during intercourse, as well as periodic cramping pain in the lower abdomen.

To make a diagnosis, it is necessary to undergo a comprehensive examination, which includes the following procedures:
- Gynecological examination - particularly large polyps can be palpated during manual examination; cervical polyps can be detected during examination in the speculum.
- Ultrasound of the pelvis - in the uterus, growth of the endometrium with a local increase in its mucous layer is detected. The structure of this neoplasm is homogeneous.
- Separate diagnostic curettage followed by histological examination of the obtained material.
- Hysteroscopy - allows you to examine the endometrium from the inside, visualize single or multiple polyps and determine their location. The procedure is also therapeutic in nature, since it allows for the simultaneous removal of all identified tumors and their subsequent histological examination. This is the most effective method for diagnosing a polyp in the uterus.
What procedures can a gynecologist perform during hysteroscopy?
Hysteroscopy is a diagnostic procedure, however, during it some additional manipulations can be performed, including therapeutic ones:
- Biopsy is a procedure during which a piece of pathologically changed tissue is removed and sent to the laboratory for histological and cytological examination. This allows you to establish a more accurate diagnosis, confirm or exclude the presence of a malignant tumor in the uterus.
- Hysteroscopy allows you to remove various pathological formations protruding into the uterine cavity, such as polyps and fibroids.
- The source of bleeding can be eliminated using electrocoagulation and low temperature (cryosurgery).
- Place contraceptive devices in the fallopian tubes.
The Euroonko clinic in Moscow offers special comprehensive programs for women, for example, hysteroscopy with separate diagnostic curettage of the cervix and uterine body. The cost of the service includes a 6-hour stay in a comfortable hospital, meals, and all related procedures.
When can hysteroscopy be performed?
Most often, gynecologists prescribe hysteroscopy in the following situations:
- Detection of atypical cells based on PAP test results.
- Vaginal bleeding between periods, postmenopause.
- Infertility is when you cannot get pregnant after a year of regular sexual activity.
- Frequent miscarriages.
- The need to clarify the condition of the uterus with scars and fibroids.
- The need to confirm or rule out certain diagnoses using biopsy.
Risks of hysteroscopy
Overall, this is a safe procedure. For two days after hysteroscopy, you may experience slight bleeding from the vagina and cramps in the lower abdomen - this is normal. More serious complications are very rare, occurring in no more than 1% of cases.
At Euroonko, the research is carried out by a highly qualified specialist - Natalya Evgenievna Levchenko, oncogynecologist, professor, doctor of medical sciences. The clinic uses equipment for hysteroscopy from the world's leading manufacturers, which allows the examination to be carried out as comfortably and safely as possible.
Complications after polyp removal
As after any gynecological operation, the following complications may develop after hysteroscopy:
- Damage to the wall or cervix - treatment may require additional surgery to close the perforation.
- Damage to the cervix - may require stitches.
- Bleeding.
- Infectious complications.
It should be noted that complications after hysteroscopy are much less common than after other gynecological interventions performed “blindly”. But the possibility of their development cannot be completely excluded.
What alternatives are there to hysteroscopy?
Hysteroscopy can be replaced by some other diagnostic procedures, but not in all cases:
- Transabdominal ultrasound of the pelvic organs through the anterior abdominal wall helps to identify diseases that lead to pelvic pain, menstrual irregularities, vaginal bleeding, and infertility.
- Transvaginal ultrasound is performed with a special probe inserted through the vagina. It allows you to obtain more informative images of the uterus and its appendages.
- Aspiration biopsy of the myometrium. This procedure does not require hysteroscopy: using vaginal speculum, the cervix is visualized and a tube connected to an aspirator is inserted through it.
All these studies are not as informative as hysteroscopy. However, if you start the diagnosis with them, in some cases endoscopic examination of the uterus may not be required. Sometimes these diagnostic methods are used as an alternative if there are contraindications for hysteroscopy for one reason or another.
Book a consultation 24 hours a day
+7+7+78
When is polyp removal necessary?
The choice of patient management tactics and determination of the need to remove the polyp is determined individually. If a woman is of reproductive age and has no symptoms of a polyp, conservative management tactics can be chosen. In this case, the patient should undergo regular monitoring.
In all other cases, removal of polyps is indicated:
- Presence of symptoms of the disease.
- Pre- and postmenopausal periods, even if there are no symptoms.