June 3, 2021 The formation of kidney stones often causes an imbalance in the acid-base balance. Before the onset of pain, a person may not be aware of the existence of stones. Phosphate kidney stones are among the most dangerous because they are prone to active growth. That is why timely diagnosis of urolithiasis and qualified treatment are so important. At the State Clinic of Urology named after R. M. Fronstein of the First Moscow State Medical University named after I.M. Sechenov, you can undergo a comprehensive examination and receive help from the best specialists in the capital.
The mechanism of appearance of phosphates in urine
Salts are formed as a result of an imbalance in the acid-base balance. During metabolism, phosphorus is converted into an acid, which subsequently combines with various elements to form phosphate salts. Typically, such formations are gradually eliminated through the kidneys and do not cause harm to the body.
With some diets and diseases, the acidity of urine changes. Under alkaline conditions, increased formation of amorphous phosphates and tripelphosphates is observed. The kidneys cannot cope with the load - they do not have time to remove all the salts, which is why they accumulate and form calculi (stones).
Phosphate salts, being in excess, interfere with the absorption of a large number of useful substances in the body, including calcium, which inevitably leads to hypocalcemia.
general characteristics
Inorganic phosphorus is one of the main mineral components of bone tissue (more than 80% of the total amount of phosphorus in the body). In cells it is part of nucleotides, nucleic acids, phosphoproteins, phospholipids, coenzymes, enzymes, ATP. Human bones consist of hydroxyapatite 3Ca3(PO4)3Ca(OH)2. The composition of tooth enamel includes fluorapatite. Metabolism of phosphorus compounds occurs in the liver. The metabolism of phosphorus compounds is regulated by hormones and vitamin D. Necessary for bone formation and to maintain cellular energy metabolism. Phosphorus metabolism in the body is closely related to calcium metabolism, therefore the ratio of calcium and inorganic phosphorus in the blood is of great diagnostic importance. Serum phosphorus concentrations exhibit a circadian rhythm (highest in the morning, lowest in the evening) and are subject to rapid changes secondary to factors such as diet (carbohydrates), the presence of phosphate-binding antacids, and changes in growth hormone, insulin, and renal function levels. Urinary phosphorus excretion is highly variable and depends on diet. There are significant daily fluctuations in urinary excretion of inorganic phosphorus, with maximum values in the afternoon. With a standard diet, changes in phosphorus excretion may be a consequence of pathological processes in the skeletal system and kidneys. Reliability of interpretation of urinary calcium and phosphate excretion tests increases with creatinine clearance
What tests detect phosphates?
Determining phosphates in urine is very simple. It is enough to pass a general urine test for salt. This is a simple and informative type of research.
Examination of the urine reveals unusual sediment, indicating problems with renal filtration. The fact that there are phosphates in the secretions is indicated by low acidity - less than 7.

To obtain detailed results about the functioning of the urinary system, a daily salt test is prescribed.
In order for the result to be as reliable as possible, a couple of days before submitting the material you must:
- eliminate physical and emotional stress;
- remove harmful foods from the diet (smoked meats, pickles, sweets);
- quit bad habits.
Other tests may be needed:
- bacteriological culture of urine;
- blood analysis;
- radiography;
- Ultrasound of the thyroid gland, bladder and kidneys.
Diagnostics
Despite the fact that crystals are quite common in normal urine, repeated detection of crystalluria requires a visit to a general practitioner to determine the cause. When interviewing the patient, the nature of the person’s diet is clarified, what medications he is taking, and whether he is registered with a dispensary. An additional examination is prescribed, including:
- General blood analysis.
The level of red blood cells and hemoglobin is examined, which can be either decreased or increased. - Blood chemistry.
In case of impaired renal excretory function, the concentration of urea and creatinine is increased; in diseases of the hepatobiliary system - ALT, AST, direct bilirubin. With gout, there is an increase in uric acid levels in the blood. Biochemical markers of hemolysis are LDH, indirect bilirubin. People with Wilson-Konovalov disease have decreased levels of ceruloplasmin and increased amounts of copper in the blood. - Analysis of urine.
Indicators of a general urinalysis (leukocyturia, hematuria, proteinuria) and other findings during microscopy of urine sediment (epithelial cells, formed elements, casts) can help in identifying the cause of crystalluria. Biochemical analysis of 24-hour urine for oxalates and calcium is the gold standard for diagnosing oxalosis. - Amino Acid Metabolism Study
. If amino acid crystals are detected, the concentration of tyrosine, leucine, cystine in blood serum and urine is measured. - Instrumental research.
If there is a suspicion of urolithiasis, a kidney ultrasound is prescribed, which can visualize stones, as well as excretory urography, which allows one to assess the presence and degree of urinary tract obstruction.
Reasons for the appearance of phosphate salts
There are several factors for phosphate getting into the urine in adults and children:
- incorrect lifestyle and diet (vegetarian menu, some diets);
- abuse of foods high in phosphorus (dairy products, seafood, whole grain cereals, mineral water);
- metabolic disease;
- lack of fat-soluble vitamins;
- pregnancy (changes in hormonal levels and taste preferences);
- dehydration due to vomiting and diarrhea;
- poisoning with chemicals containing phosphorus.

Amorphous phosphates in the urine of a child under 5 years of age usually indicate immaturity of the digestive system and mechanisms for regulating metabolic processes.
Phosphates and other salts in urine can be a sign of various diseases:
- genetic disorder - phosphate diabetes;
- Fanconi disease;
- urolithiasis (stones in different parts of the urinary system);
- chronic kidney failure;
- renal tubular acidosis or congenital anomaly;
- hyperfunction of the thyroid and parathyroid glands.
Often the amount of phosphates in the urine increases with inflammatory and infectious diseases of the genitourinary system:
- cystitis;
- pyelonephritis;
- urethritis;
- prostatitis.
Reasons for education
- Violation of water-salt balance with low fluid intake.
- Urinary tract infection.
- Phosphaturia is the rapid transformation of phosphates into crystals.
- Slow urine formation with high salt concentrations;
- deficiency of vitamins D and A;
- Love of chocolate, tea and coffee, as these habits cause an increase in calcium levels in the blood;
- physical inactivity;
- increased calcium content in urine due to poor diet;
- endocrine diseases;
- genetic predisposition;
- kidney dysfunction.
Additional symptoms of phosphaturia
Mild phosphaturia can go undetected for a long time, especially when its cause lies in diet and is temporary. But if the deviation is caused by one of the diseases, then specific signs will be added to the general signs, indicating a high level of phosphate salts in the urine.
The main symptom is cloudy urine with the formation of sediment and flakes. If you ignore the problem for a long time, other signs of the disease may appear:
- nausea and vomiting;
- aching pain in the lumbar area (especially after physical activity);
- flatulence;
- intestinal colic;
- false urge to defecate;
- frequent urination;
- incomplete emptying of the bladder;
- pain in the stomach, back, groin:
- low-grade fever (with chronic pyelonephritis).
Definition and Causes
In this section we will talk about phosphaturia, that is, excess phosphorus in the urine, and what it can be.
Surprisingly, urine is a unique liquid that cannot be obtained in inanimate nature. Poorly soluble compounds, which include phosphates and phosphoric acid salts, are or can be found in the urine in such a high concentration that several times exceeds their maximum solubility in water. How is this possible? How can urine, being water enriched with salts, deceive nature?
This possibility is associated with the high alkaline reaction of urine, and with the presence of special protective colloidal proteins that can keep poorly soluble lime phosphate salts in dissolved form. But humans are not the leader here, since the greatest ability to dissolve phosphates in urine is possessed by herbivorous ungulates, whose urine is always alkaline. The urine of people who have been on a vegetarian diet for a long time can be compared with the urine of herbivores in terms of alkaline capacity.
How often does it happen that there is a lot of phosphate in the urine, both crystals and amorphous salts? Here are the statistics. Oxalaturia, or calcium release, is 85% of all cases, and phosphaturia accounts for 10%. However, one should not think that calcium phosphate is released exclusively in pure form. Most patients with excess phosphorus in the urine excrete it not only in the form of calcium phosphate, but also with calcium oxalate, that is, oxaloacetic salt. In the case of high concentrations of uric acid, the remaining small percentages account for, together with cystinuria.
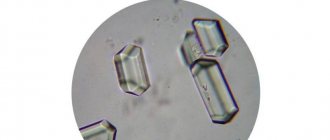
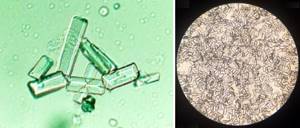
In addition to amorphous phosphates, so-called tripelphosphates can also be observed in the urine. What it is? This is a crystalline phosphate, in which, in addition to calcium and phosphorus, there are also magnesium and ammonium ions, that is, NH4, which give an alkaline reaction to the urine. They are clearly visible under a microscope, and after centrifugation, sometimes the entire field of view is completely occupied by these crystals.
In the previous section it was said that phosphaturia may be associated with changes in the concentration of phosphorus in the blood plasma, or with kidney pathology. Such conditions are called primary, or true phosphaturia. It is quite possible that the parathyroid glands work well, the person does not have any oncology, he does not have kidney pathology, renal failure or tubular necrosis, and he has a lot of phosphorus in his urine. Why?
Urological pathology or a chronic infection of the genitourinary system, for example, long-term chronic pyelonephritis, is to blame. Reproducing microorganisms have high urease activity and produce the enzyme urease. It decomposes urea, and as a result, the urine begins to alkalize. In the article about the dissolution of urinary stones, we wrote that alkalization of urine leads to the dissolution of urates, but if you overdo it a little with medications, the urine reaction will become so alkaline that, despite the dissolution of urates, it will begin to precipitate phosphates, which are even more difficult to dissolve , than urates.
This is precisely the situation, “woe from mind,” that occurs in the case of a chronic infection: the patient does not seem to have any signs of urolithiasis, does not take alkalizing drugs, but microorganisms are to blame for the excess of alkaline urine. It is enriched with magnesium ammonium phosphate, so-called struvite stones, which are markers of kidney infection. If struvite stone combines with carbon dioxide apatite, then the same tripolyphosphate will appear.
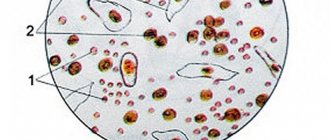
How to translate all this chemical wisdom into simple language? Very simple. If we talk about adults, phosphaturia is most often observed in patients with long-term diabetes mellitus, alcoholism and the presence of a chronic urinary infection. Many amorphous crystals in the urine appear as cloudy, milky white urine. These are all salts of phosphate of lime, which, soon after urination, immediately fall out of the urine in the form of sediment.
Old doctors have noticed that such phosphaturia can occur after the release of a large amount of acidic gastric juice, for example, when studying stimulated secretion.
Phosphaturia occurs after numerous vomitings of acidic masses, due to the loss of hydrochloric acid. Accordingly, if the body loses its acid potential, its alkaline reserve increases, and alkalization of urine leads to increased excretion of phosphates. Such frequent vomiting occurs in patients with chronic alcoholism.
In order to detect phosphates and crystals in urine, or more precisely to suspect their presence, you can carefully examine your own urine in a jar after it has completely cooled. It is then that a whitish cloudiness can be noticed, and this will be enough to collect daily urine and take it to the laboratory. How daily urine collection is carried out, and according to what rules - a separate article is devoted to this.
Also, old doctors knew the sign of phosphaturia in the form of the appearance of a very light, whitish, slightly greasy-looking, opalescent film that appears at the point of contact of the surface of cooled urine with the wall of the vessel. This film indicates a high concentration of phosphates, and its visibility increases as the sediment increases.
Let us remind you once again about the primary causes of high phosphorus in the urine, which are not related to urinary infection and poor kidney function. This:
- hyperfunction of the parathyroid glands, including their adenoma;
- metabolic acidosis, which develops with any severe multiple organ pathology, for example, with diabetes mellitus;
- bone fractures, characteristic, among other things, of multiple myeloma and oncohematological pathology;
- significant excess of vitamin D;
- Fanconi syndrome, in the case of familial hypophosphatemia;
- due to taking certain medications. These include, in addition to vitamin D, furosemide, parathyroid hormone, glucocorticosteroids, and other urine alkalizing substances, for example, excess regular baking soda to combat heartburn.
When is treatment needed?
The need for therapy is determined individually. Treatment methods directly depend on the reasons that caused the increase in phosphate salts in the urine. Initially, the patient is prescribed a full examination, including ultrasound of the urinary system.
In uncomplicated cases, the problem is solved using the following methods:
- taking medications;
- physiotherapy;
- dietary ration;
- additional multivitamin complex;
- kidney cleansing using diuretic herbs;
- exercise and exercise.
A person needs to watch what he eats. The menu should be varied and balanced. It is advisable to remove fatty meat, fish, milk and cottage cheese, chocolate, sweet fruits, beans, marinades, sauces, ketchup and spices from it.

Only a specialized doctor has the right to prescribe treatment. It is necessary to adhere to all recommendations regarding dosages and timing of therapy. Self-medication is dangerous and can lead to complications.
Treatment of the disease
The goal of therapy is to dissolve the stones. The problem is solved by a set of measures.
- In the presence of infectious diseases, antibacterial, antimicrobial and anti-inflammatory treatment is carried out - antibacterial and sulfonamide agents are prescribed.
- It is possible to take herbal remedies and medications to dissolve the formations. IMPORTANT! Before use, be sure to consult with a specialist who will conduct the necessary examinations to determine the type, size and location of the stones. Those fees that will be useful for phosphate stones can be harmful for other types of stones and vice versa. Don't self-medicate!
- For pain, antispasmodics are prescribed.
- Treatment includes a special set of exercises and diet.
If all doctors' recommendations are followed, kidney stones are quickly removed without pain. If the dissolution process is delayed, lithotripsy is used - a shock wave method. If the kidneys are in advanced condition, the patient is recommended to remove the formations surgically.
Prevention of phosphaturia
Prevention is of great importance in maintaining health. To prevent phosphaturia, you must follow a number of rules:
- Limit the consumption of preservatives, spicy, salty and smoked foods.
- Drink at least two liters of fluid per day.
- To live an active lifestyle.
- Avoid hypothermia.
- Once a year, submit urine for laboratory testing.
- If you experience lower back pain, consult a doctor.
Due to the high vulnerability of children to various harmful factors, doctors advise taking into account the recommendations of specialists when preparing a diet and regularly visiting a pediatrician.
Patient preparation rules
Random urine sampleStandard conditions:
Biomaterial is accepted during the working day of the departments of ML "DILA".
Any portion of urine, regardless of the time of day. The material is collected after toileting the external genitalia. Urine (daily)Standard conditions:
Biomaterial is accepted during the working day of the departments of ML "DILA".
The morning portion of urine is placed in the toilet. Collect urine for a day, including the morning portion of the next day, into a clean urine collection container. After the last urine collection, mix all collected urine, determine its volume and record it. Pour 100 ml and deliver to the nearest branch of ML “DILA” within 2 hours. Keep the container with biomaterial in a cool place, protected from light, during collection. Possible:
To collect daily urine, the patient is asked to purchase a 2-liter container at the price price (the cost of the container is not included in the cost of the study).
You can add this study to your cart on this page
Treatment
How to treat phosphates in urine? First of all, you need to eliminate or eliminate the cases described in the previous paragraph, and then phosphorus in the urine will return to normal.
But if we are talking about symptomatic, secondary forms of phosphate crystalluria, then the treatment should be the opposite of the treatment of urate stones. Then the urine had to be alkalized, but now it needs to be acidified. For this purpose, treatment with mineral waters is used, the drugs prescribed are Cystenal, Methionine, and ascorbic acid.
It is quite possible to reduce the absorption of phosphorus and calcium in the intestine by prescribing antacid drugs, for example, Almagel is used.
If tripelphosphates or struvite stones are found in the urine, then it is imperative to treat the secondary urinary infection and sanitize the lesions in the urinary system. Rational diet therapy can be considered the basis of treatment.