What it is
CRP is a blood plasma protein whose concentration increases during inflammation.
The bulk of the protein is produced in liver cells in response to certain signals from macrophages (immune cells)¹. The main function of SRB is protective. It activates the complement system (a group of proteins with antibacterial activity), as well as some cells of the immune system. The concentration of CRP increases in proportion to the scale of the inflammatory process. The more inflammation, the more protein is produced in the liver.
When inflammation becomes chronic, the level of CRP decreases (sometimes to zero). However, during exacerbations it rises again.
Another property of CRP is the binding of low-density lipoproteins (LDL)². This is the so-called “bad cholesterol”. Thus, this protein also contributes to the development of atherosclerosis. An increase in C-reactive protein concentrations in the absence of acute infection or injury may indicate a risk of cardiac pathologies.
Blood test for C-reactive protein

Blood to determine the level of C-reactive protein is taken from a vein.
Photo: freepik.com As a rule, C-reactive protein is determined in a biochemical blood test (CRP). The indicator is measured in milligrams per liter (mg/l). Blood for this analysis is taken from a vein.
Normal CRP values may vary between laboratories. In most cases this is up to 1 mg/l. In some institutions - up to 5 mg/l. There is no lower limit for this marker, since the protein is determined in the acute phase of inflammation.
CRP or ESR?
Many of us are familiar with such an analysis as ESR - erythrocyte sedimentation rate. This is another marker of inflammation, but not as accurate and specific as CRP. The C-reactive protein test has several advantages over ESR, namely:
- CRP increases within a few hours after the onset of inflammation. It decreases faster with anti-inflammatory therapy. If pathological ESR levels last up to 2-4 weeks after inflammation is eliminated, then CRP lasts up to 10 days.
- CRP indicators do not depend on gender (the same for men and women), the number of red blood cells per unit volume of blood and time of day. And these factors influence ESR.
Blood test total protein
Proteins are a substance that predominates in the composition of the dense residue of blood serum. They are the main building material of all cells and tissues in the body. Proteins also make up enzymes, hormones, antibodies, and blood clotting factors. Proteins are also responsible for transporting hormones, vitamins and minerals, fat-like substances, as well as other metabolic components in the blood. Another important role of proteins is the transport of all of these substances into cells. The amount of proteins in the blood serum directly affects the osmotic pressure of the blood, which is responsible for the balance between the water content in the body tissues and inside the vascular bed. Osmotic pressure is also responsible for maintaining tissue elasticity. Proteins play a key role in ensuring acid-base balance in the body. Proteins are also the main source of energy during malnutrition or starvation.
Serum proteins are of two types: albumins and globulins. The former are synthesized by the liver from incoming food. Albumin concentration affects the level of osmotic pressure. Globulins are the basis of immunity, ensuring normal blood clotting. Globulins are also contained in enzymes, hormones, and carrier proteins of various biochemical compounds.
Several physiological conditions of a non-pathological nature, as well as a number of diseases, can cause changes in protein levels in the blood. There are two types of deviation in blood protein levels: relative and absolute.
Explanation of the analysis for Total protein
Determination of total protein in blood serum is used to diagnose diseases of the liver, kidneys, cancer, and nutritional disorders.
The normal level of total blood protein is 64–83 g/l.
Increased protein content occurs in acute and chronic infectious diseases, cancer pathology, blood diseases, and dehydration. A decrease in protein levels is most often caused by diseases of the liver, kidneys, intestines, starvation and some others.
Indications
CRP in the blood is determined under the following circumstances:
- Symptoms of acute infectious diseases. These include high body temperature, headache, cough, urinary disorders and others.
- As part of a comprehensive examination of healthy individuals, especially the older age group (over 45 years old). This is done for preventive purposes.
- When examining patients with cardiovascular diseases (for example, coronary heart disease or hypertension).
- Examinations for acute myocardial infarction.
- As part of a comprehensive examination of people with chronic diseases such as diabetes, atherosclerosis or severe renal impairment. Based on the CRP level in such people, the risk of cardiovascular complications can be determined.
- In control studies to evaluate the effectiveness of treatment of cardiovascular pathologies. In particular, this is done when taking aspirin and statins in patients with atherosclerosis.
- Inflammatory processes of any origin. In addition to infectious pathologies, these are also parasitic, tumor diseases and injuries.
- Control tests to evaluate the effectiveness of antibacterial therapy for infectious diseases.
results
According to anamnestic data, it was found that only 4 (9%) children were diagnosed with ASD before the age of 3, in 8 (17.5%) - by 4 years, in 16 (35.5%) - by 5, in 11 (24.5%) - by 6 and in 6 (13.5%) - by 7. Thus, in the group of children we examined, the diagnosis of ASD was made in a timely manner in 12 (26.7%) children, which made it possible to begin treatment in a timely manner -corrective measures (timely diagnosis up to 4 years), and in 33 (73.3%) children the diagnosis was determined by 5-7 years, which can be attributed to late diagnosis.
Analysis of the most significant risk factors associated with autism showed that their share in the MG of children with ASD was significantly higher than in healthy children in the control group, and that in most cases there was a combined effect of several factors (Fig. 1).
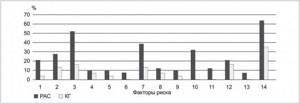
Rice. 1. The proportion of the main risk factors in children from the OG and CG. 1 - presence of autism, other forms of ASD, schizophrenia and other psychoses, affective disorders and other mental and behavioral disorders in a family history; 2 - mother’s age over 40 years at the time of conception; 3 - father’s age over 40 years at the time of conception; 4 - infectious diseases during pregnancy; 5—threat of miscarriage in the first 20 weeks of gestation; 6 - conception using in vitro fertilization; 7 - signs of asphyxia during childbirth (low Apgar score), as well as resuscitation measures after birth; 8 — obstetric operations (caesarean section); 9 — prematurity (gestational age less than 38 weeks); 10 - congenital brain defects; 11 — congenital malformations of other organs; 12 — maternal smoking; 13 - taking valproic acid, antidepressants, antibiotics during the year before pregnancy and/or during pregnancy; 14 - living in big cities and their suburbs.
The following factors had the greatest weight in the development of ASD: the age of the father and mother over 40 years at the time of conception of the child - in 23 (51.1%) and 12 (26.6%) cases, respectively; signs of hypoxic-ischemic brain damage during pregnancy and childbirth, as evidenced by a low Apgar score (below 6 points), and resuscitation measures (stay in the neonatal intensive care unit) - 17 (37.7%); the presence of malformations of the brain (according to MRI data taken at the place of residence) - 14 (31.1%); maternal smoking - in 9 (20%).
The majority of patients - 28 (62.2%) - lived in large cities or their suburbs. When talking with the parents of children in the study group, it was found that many relatives had disorders of expressive speech, speech articulation, some had severe mental illness (schizophrenia, bipolar disorder, autism), some parents noted that their relatives had depressive or affective conditions, epilepsy - 9 (20%) cases.
The representation of other risk factors is not so high, but they play a significant role in the risk of developing ASD. Thus, infectious diseases during pregnancy (acute respiratory viral infections, bronchitis, pneumonia, exacerbation of chronic diseases such as cholecystitis, pyelonephritis, sinusitis, chlamydia, carriage of cytomegalovirus, herpetic infection) were present in the anamnesis of 4 (8.8%) mothers. There was a threat of miscarriage in the first half of pregnancy in 4 (8.8%) cases, children with ASD born through in vitro fertilization (IVF) were noted in 3 (6.6%) cases. However, the fact of IVF is closely related to an unfavorable obstetric history, and this manipulation is carried out, as a rule, when the mother’s age reaches 35 years or older, therefore, in our opinion, the mother’s health condition and her age at the time of IVF are more important. Delivery by cesarean section was in 5 (11.1%) mothers, the birth of a child at a gestational age of less than 38 weeks was detected in 4 (8.8%) children, congenital malformations of organs, mainly the heart, genitourinary system and gastrointestinal tract, were in 5 (11.1%) children. The mother took valproic acid, antidepressants, and antibiotics in the period before conception and during pregnancy in 3 (6.6%) cases, which must be considered in terms of not only the action of the pharmacological drugs themselves, but also the pathology present in the mother, in connection with which these medications were used (affective states, depression, epilepsy, moderate infectious diseases and exacerbation of chronic diseases).
When assessing the average content of S100B protein in the blood serum of children from the OG group, its significant increase was noted in comparison with that in children from the CG ( p
=0.005). In 14 (31%) children with ASD, S100B values were slightly higher or at the upper limit of normal, in contrast to children in the control group, of which 9 (20%) had abnormalities of brain structures, 5 (11%) had no neuroimaging signs of brain damage was.
In order to identify as few latent common factors as possible that accurately describe the observed associations between ASD risk factors and S100B protein, we conducted a factor analysis. Previously, to select variables for factor analysis, a correlation analysis was carried out, which made it possible to identify a complete and non-redundant set of features by combining highly correlated features.
Significant factors in the model were examined using the scree-test and the Kaiser criterion; the 2 most significant factors in the studied model were identified. When analyzing the space of common factors, in order to both maximize the magnitude of factor loadings of the selected factors and achieve the most “interpretable” solution, factors were rotated using the biquartimax method applied to the original factors. In table 1 are given
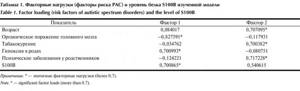
Table 1. Factor loadings (ASD risk factors) and S100B protein level of the studied model Note. *—significant factor loadings (more than 0.7). loadings of factors selected by correlation analysis (other risk factors that did not have reliable factor loadings were omitted and not indicated).
The described variance is 36.3%, with the largest percentage of organized variance accounting for factor 1 - 19.5% [expl. Var.=3.3188 (variance), Prp. Totl=0.1952 (share of variance)], the significance of the second factor is 16.8% [expl. Var.=2.8579 (variance), Prp. Totl=0.1681 (proportion of variance)].
Using the method of descriptive statistics (for visual presentation and analysis of the results of the entire study sample, CG and CG), the S100B levels in the blood serum of children with autism and CG were studied. Serum levels of S100B protein in children with autism are presented in Table. 2
.
In the group of children with ASD who had MRI abnormalities in the development of brain structures (MRI group (+)), the levels of protein S100B were significantly higher compared to those of children in the control group ( p
=0.002), as well as children in the ASD group who do not have pathology according to MRI [(MRI group (–)),
p
1 = 0.002 (Table 2)]. The levels of this protein in children with autism without disorders of brain structures did not differ significantly from those of healthy children.
An assessment of the S100B protein content depending on the severity of autism showed that in severe cases of the disease its values were significantly higher than in the control group ( p
=0.003), and with moderate severity this indicator did not have a significant difference in comparison with healthy peers. There was no significant difference between the indicators of groups of children with ASD with moderate and severe degrees of severity.
To analyze the influence of the severity of the disease and the presence of organic brain damage on the content of the S100B protein in children with autism, factorial analysis of variance (ANOVA) was performed. The results of the analysis of variance of the relationship between S100B content in children with autism and the severity of the disease did not show a statistical relationship - F1/1 df=3.459, p
=0.07 between the studied indicators, and the content of S100B and the presence of organic brain damage according to MRI revealed a statistically significant dependence of the indicators - F1/1 df = 8.572,
p
= 0.005. Graphically, the dependence of the S100B indicator in children with autism on the presence of organic brain damage is presented in Fig. 2.
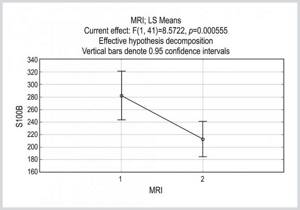
Rice.
2. Dependence of the S100B indicator in children with autism on the presence of organic brain damage. Along the MRI axis: 1 - there are malformations of the brain according to MRI data; 2 – there are no abnormalities in brain structures according to MRI data. Thus, in the presence of abnormalities in the structure of the brain (1), the amount of protein S100B in children with autism is significantly higher than in children in group (2) without abnormalities in the structure of the brain. Thus, multifactor analysis made it possible to identify the two most significant factors from the many considered. The first factor can be conditionally called the “hypoxia factor”, since its component indicators are clearly distinguished - organic brain damage, the level of S100B protein and hypoxia during childbirth. The second factor can be designated as a genetic factor, or a factor of possible mutations. Its main components are the patient’s age, the presence of mental illness in relatives, and maternal smoking during pregnancy. The initial content of glial protein S100B in children with autism (according to analysis of descriptive statistics) was significantly higher in comparison with healthy peers. The level of the studied indicator, depending on the presence of abnormalities in the development of brain structures, showed its increase in children with the presence of pathology relative to not only healthy children, but also children without signs of disorders of brain structures. In severe ASD, S100B protein levels were higher, and in moderate severity, they did not differ significantly from those of healthy peers.
However, according to analysis of variance, the content of the S100B protein was statistically dependent only on the presence of organic brain damage (according to MRI) and did not depend on the severity of the clinical manifestations of autism.
Preparing for analysis
No special preparation is required from the patient. It is necessary to comply with the standard requirements that apply before donating blood from a vein:
- You need to donate blood on an empty stomach, after 12-14 hours of fasting. As a rule, blood is donated in the morning. The last meal the day before should be 4-6 hours before bedtime. After dinner and until blood donation (the next day), only drinking clean water (not tea, coffee, juices or other drinks) is allowed.
- During the day before donating blood, you should refrain from drinking alcoholic beverages (including beer). Heavy physical activity is also undesirable.
- Your doctor may tell you to stop taking certain medications 1-2 days before donating blood (if possible). If it is impossible to cancel the medicine, then the decoding of the received data is done with a correction for this circumstance.
- You should refrain from smoking 1-3 hours before donating blood. Also avoid stress, anxiety, fast climbing stairs and any heavy physical activity.
Important: what can affect the result
Certain circumstances may distort the results of the study. You risk receiving false data if:
- took oral contraceptives the day before;
- are on hormone replacement therapy;
- are taking beta blockers, glucocorticoids, non-steroidal anti-inflammatory drugs or statins;
- recently had intense physical activity;
- you have bad habits that are difficult to give up in order to obtain correct analysis data.
Total protein
Proteins are the main building material for cells and tissues and are part of the entire body. They form a structural part of most organs; they also include enzymes and hormones that regulate all physiological processes. Two classes of proteins are constantly present in blood plasma: albumins and globulins. Albumin makes up about 60% of the total protein in the blood. It is produced in the liver and performs many functions, including being a carrier of small molecules and ions of substances, a source of amino acids for tissue metabolism, and a major component involved in maintaining osmotic pressure. The remaining 40% of blood proteins are globulins. These include enzymes, antibodies, hormones, carrier proteins, etc.
In what cases is research usually prescribed?
The test for total blood protein is part of the screening biochemical panels that are prescribed as part of a medical examination, medical examinations, during hospitalization, after illnesses, etc. to assess the patient's general health. Used as a diagnostic test to evaluate liver and kidney function
If the result is abnormal, further testing must be done to determine which specific type of protein is outside the normal range so that a specific diagnosis can be made. Such tests may include albumin and protein fractions (protein electrophoresis).
What do the test results mean?
The results of a general blood test are usually considered along with the results of other tests and can give the doctor information about the patient's overall health.
Low levels of total protein observed in liver or kidney disorders are most often associated with either insufficient synthesis or loss of protein in the body. These conditions include liver failure, fasting, celiac disease, malabsorption, inflammatory bowel disease, kidney disease
High total protein levels may be observed at a certain stage of ongoing inflammation or may be associated with a number of hematological and oncological diseases (for example, multiple myeloma, etc.).
Test deadlines.
Usually results can be obtained within 1-2 days.
How to prepare for the analysis?
No special preparation is required. You can take the test 3 hours after eating or on an empty stomach.
Norm C-reactive protein by age and gender
Since C-reactive protein is determined in the blood in response to acute inflammation or an infectious process, its level does not depend on the gender or age of the patient. This means that there are common criteria for assessing DRR for men, women and children.
To assess infectious and inflammatory processes in the body, a CRP level of up to 5 mg/l is considered normal. As for assessing cardiovascular risks, the indicators are different:
- less than 1 mg/l – low risk;
- 1-3 mg/l – average;
- more than 3 mg/l – increased.
People with elevated CRP but normal LDL levels have been found to have a greater risk of developing cardiovascular disease than people with normal CRP but elevated LDL. Thus, the CRP indicator in the prognosis of cardiovascular pathologies is much more important than cholesterol levels.
C-reactive protein and pregnancy
During pregnancy, a woman's immune system becomes more stressed.
Therefore, during this period, the level of CRP is slightly elevated. Most often this occurs from 16 to 28 weeks of pregnancy. Then the indicators gradually return to normal. The second time, an increase in CRP is possible immediately before childbirth. High concentrations of CRP in the blood during pregnancy may indicate a risk of late toxicosis. In this case, you need to consult a doctor and conduct other tests.
During pregnancy, C-reactive protein is slightly elevated. Photo: standret / freepik.com
There are (not) too many proteins
Protein is one of the most important nutrients on which the quality of the body as a whole depends. It helps restore tissue, transport oxygen throughout the body, regulate cellular metabolism, and recover from injuries and physical activity.

The amount of protein needed to maintain the body depends on several factors. Let's look at them in more detail.
Age
Everyone needs proteins, especially older people. As they age, they lose muscle mass, and this must be compensated for with nutrition: a third of the daily diet of people over 50 years old should come from proteins.
Lifestyle
The more often you play sports, the faster microtraumas appear in the muscles. For a quick recovery, you need to consume at least 200–250 grams of foods containing protein.
Weight

Men and women have different body weights, so the former, as a rule, are advised to lean heavily on proteins.
However, this does not mean that the latter should forget about them. So, summing up all the facts, we come to the following conclusion: a woman aged 28–35 years, who weighs approximately 60 kilograms and exercises 2–3 times a week, needs 70–118 grams of protein per day.
Related reading:What you need to know about the reverse diet
Causes of elevated C-reactive protein
The main reasons for increasing CRP include:
- Acute bacterial or viral infections. It has been established that during bacterial infections the amount of CRP in the blood is higher than during viral infections.
- Exacerbation of chronic infectious and inflammatory diseases.
- Malignant tumors and/or metastases.
- Tissue damage. For example, trauma, acute myocardial infarction, burns or consequences of surgery.
- Sepsis.
- Chronic, low-grade inflammatory processes (usually in blood vessels), increasing the risk of cardiovascular diseases.
- Overweight and obesity³.
- Autoimmune diseases (rheumatoid arthritis, systemic vasculitis).
- Insulin resistance, prediabetes and diabetes mellitus.
- Disorders of blood lipids (atherogenic dyslipidemia).
- Endocrine diseases and hormonal imbalance.
- Smoking and alcohol abuse.
Figure 1. Causes of elevated C-reactive protein levels.
Elevated C-reactive protein in coronavirus
Research on CRP levels has taken on added significance during the COVID-19 pandemic. The marker is considered as the main indicator of the activity of the inflammatory process in the lungs. Determination of CRP in patients with COVID-19 allows us to evaluate the following indicators:
- The severity of the disease. If a CRP level of 10 mg/l or more is determined, this indicates a moderate course of the disease. In severe cases, CRP can increase to 100 mg/l or more. At the same time, the level of CRP correlates with the volume of damage to the lung tissue.
- Monitoring of moderate and severe patients. The CRP level is determined within 24 hours after the patient is admitted to the hospital. Then, in moderately severe patients, the analysis is carried out 2 times a week, and in severe patients - every 48 hours.
- Monitoring the patient's condition with ARDS. In acute respiratory distress syndrome (ARDS), CRP levels are determined every 2-3 days. An improvement in condition is judged by a persistent decrease in the indicator.
- Development of macrophage activation syndrome (MAS). This is a serious condition that threatens the patient's life. An increasing level of CRP (in combination with some other markers) may indicate the development of MAS.
The indication for discharge from hospital is a CRP level of less than 10 mg/l.
In every second patient with coronavirus, C-reactive protein increases in the first days of the disease. Photo: halfpoint/Depositphotos
Material and methods
A single-center, non-randomized, open-label, controlled, prospective study was conducted between March 2015 and December 2021.
In the context of rehabilitation sanatorium-resort treatment on the basis of the specialized psychoneurological department of the Evpatoria Military Children's Clinical Sanatorium named after. E.P. Glinka examined 45 children, 13 girls and 32 boys with ASD (ICD-10 category F84.0-F84.9), aged from 6 to 15 years (average age 10.3±2.5 years). They made up the main group (MG).
The criteria for inclusion of children in the study were an established diagnosis of ASD and the presence of disability for this disease. The criterion for non-inclusion was comorbid pathology - epilepsy (G40) with remission for less than 3 years.
The control group (CG) included 25 children of health groups I and II who underwent health improvement at the Evpatoria resort.
In all cases, voluntary informed consent was obtained from the child's parents to conduct the study.
We conducted a comprehensive examination of the OH with a detailed collection of anamnesis from the child’s mother, obtaining the necessary information from medical records, examining the children by a psychiatrist, pediatrician, neurologist, psychologist, speech therapist and using clinical, functional and laboratory methods.
For each patient, a special card was filled out, which reflected formal information, as well as data from the medical history (study of the lifestyle and health status of the parents for 1 year before conception, mental illness of relatives, age of the parents, course of pregnancy, childbirth, course of the postpartum period, psychomotor child development), time of onset of the disease and diagnosis, features of the formation of clinical symptoms, previous diagnosis (psychological examination and MRI).
Disease severity was assessed using the Children's Autism Rating Scale (CARS) for children from 2 years of age. Scores from 30 to 37 (mild or moderate autism) were determined in 28 (62.2%) children and 37-60 points (severe autism) in 17 (37.8%).
Biochemical studies included determination of S100B protein in blood serum using the CanAg S100 EIA FUJIREBIO enzyme immunoassay kit (Diagnostics, Inc., Sweden) to quantify human S100B in blood serum.
Statistical data analysis was carried out using the Statistica v software package. 6.0 (StatSoft Inc., USA). The description of quantitative characteristics is carried out using the median (Me) indicating the interquartile range (Q1; Q3), where Q1 is the 25th percentile and Q3 is the 75th percentile, standard deviation (σ). Comparative analysis of quantitative variables was carried out using t
-Student's t-test for independent samples.
Differences were considered statistically significant at p
<0.05. Based on the objectives of the study, the presence and degree of influence of the hypothesized factors on the final result expressed in the studied set of variables was assessed using factorial analysis of variance (ANOVA). In order to discover hidden common factors that explain the relationships between the observed characteristics, factor analysis was carried out. The number of factors was determined using the Kaiser criterion and the scree test. To identify factors, the principal component method was used. After finding the space of common factors, the factor loadings were rotated both in order to maximize the magnitude of the factor loadings of the selected factors and to achieve the most “interpretable” solution. Rotation was carried out using the varimax, biquartimax, quartimax, equimax methods, which were applied to both the original and normalized factors [26].