Using a general blood test, the doctor can determine the condition of the patient’s different organs and systems. After all, blood comes into contact with all tissues of the body and serves to transport metabolic products and oxygen. In order to correctly diagnose pathology, the analysis requires assessing not only the quantitative characteristics of blood cells, but also their quality. It is especially important to determine the condition of red blood cells. Several indicators are used for this, one of them is RDW. This is a fairly important indicator that allows us to identify many pathologies, primarily various types of anemia. But most people don't know what it means, so questions often arise when receiving blood test results.
The erythrocyte distribution index RDW SD is decreased or increased in a child, normal in a blood test
A general blood test is a mandatory diagnostic procedure for children.
It allows you to get acquainted with the characteristics of erythrocytes, leukocytes, platelets: their number, erythrocyte, leukocyte and platelet indices.
One of the parameters that UAC shows is RDW. Let's consider what this indicator means and whether you should worry if it is elevated or decreased in children.
RDW and its varieties
What is RDW? The abbreviation stands for Red Cell Distriburion Width. This is one of the general clinical blood test indices, indicating the distribution of red blood cells by volume. By deciphering the index readings, the laboratory technician identifies the presence of red blood cells, which vary in shape and size.
The task of red blood cells is to transport hemoglobin along with oxygen molecules. Successful functioning depends on the shape of the cell - a biconvex disk. The change in volume is called anisocytosis.
There are two varieties of RDW:
- rdw-cv - shows the severity of anisocytosis;
- rdv-sd - indicates the difference between the sizes of red blood cells.
RDW has a direct correlation with another UAC indicator - MCV. MCV index is the average volume of the red cell.
Purpose of the analysis
The erythrocyte index is included in the UAC. The attending physician can purposefully send a patient to donate blood if the following ailments are suspected:
- oncological pathologies;
- iron deficiency anemia;
- diabetes mellitus;
- liver damage.
Diagnosis of the erythrocyte count is indicated for the following symptoms:
- hereditary predisposition to thalassemia;
- lack of iron in the body;
- weakness, dizziness, hyperhidrosis and other signs of anemia;
- infectious diseases with a long course;
- profuse blood loss.
With pathologies of the form, blood cells cannot perform their main function - to carry oxygen to organs and remove waste products. RDW shows the percentage of red blood cells with a changed shape.
Normal indicators
What indicators are considered normal? The table provides information with a breakdown of the values of two types of index for children and adults:
| No. | Index | Meaning |
| 1 | RDW-SD | 39-46 femtoliters |
| 2 | RDW-CV | Adults - 10.9-15.6% |
| Children - 15-19.1% |
In some cases, additional diagnostics are required, since the value remains normal in some ailments:
- Spherocytosis. A hereditary pathology in which red blood cells are round rather than biconcave.
- Aplastic anemia. Stopping the growth and maturation of cells in the bone marrow. Without treatment, patients die within a few months.
- Some types of hemoglobinopathies. A congenital disorder of the structure of the hemoglobin protein, which causes pathology of red blood cells. This class of diseases includes sickle cell anemia and thalassemia.
What do increased readings mean?
The RDW index is elevated - what does this mean? An increase in the distribution of red blood cells by volume indicates various ailments of the circulatory system. To make a correct diagnosis you should always look at the MCV. The table shows the breakdown of analyzes when RDW is increased, depending on the MCV indicator:
| № | MCV increased | MCV is normal | MCV reduced |
| 1. | Liver damage due to alcohol abuse | The onset of iron deficiency anemia is a violation of hemoglobin synthesis due to a lack of iron in the body. | Iron-deficiency anemia |
| 2. | Hemolytic anemia - increased destruction of red blood cells | Macrocytic anemia | Thalassemia - decreased formation of polypeptide chains included in the structure of hemoglobin |
| 3. | Megaloblastic anemia due to deficiency of cyanocobalamine and folic acid. It is characterized by the presence of immature red blood cells - megaloblasts - in the hematopoietic brain. | — | — |
| 4. | Retinol hypovitaminosis | — | — |
What does it mean if the indicator is reduced?
What does it mean when RDW is below normal? As with an upgrade, if it's downgraded you should look at the MCV value:
- low MCV - pathology of the liver or spleen;
- high MCV - cancer lesions with metastases to the bone marrow.
If the index is down slightly, then you probably don't need to worry. It can fluctuate due to hormonal fluctuations during menstruation, after drinking alcohol or fatty foods. In infants the rate is slightly lower. This is normal and goes away after a few weeks; parents should not worry about their child.
Reasons for increasing RDW
Nutrient deficiency
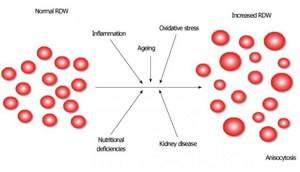
Deficiencies of various nutrients can cause an increase in RDW, for example:
- Iron deficiency [r, r, r, r]
- Folic acid deficiency [R]
- Vitamin B12 deficiency [r, r]
This is because your body needs these nutrients to produce healthy red blood cells. Any of these deficiencies can eventually lead to anemia.
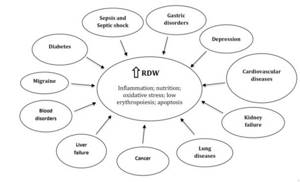
Inflammation
Some studies suggest that higher RDW values are associated with inflammation and higher levels of inflammatory cytokines such as IL-6, IL-8 and TNF-alpha. [r, r, r, r, r, r, r]
Inflammatory cytokines can interfere with red blood cell production and thereby increase RDW. Additionally, oxidative stress, which often accompanies chronic inflammation, can reduce red blood cell lifespan and further increase RDW values. [R, R]
High RDW has been found in people with diseases associated with inflammation, such as inflammatory bowel disease, celiac disease, polycystic ovary syndrome (PCOS), and major depressive disorder (MDD). [r, r, r, r]
REASONS FOR INCREASING RDW
Sleep disorders
In a study of 17,500 adults, those who slept less or more than 7-8 hours a night were more likely to have high RDW values. This was especially true for people who slept 10 hours a night - their chances of having increased RDW increased by almost 70%. [R]
RDW values are higher in people with sleep apnea. [r, r]
RDW scores were also associated with shift work with circadian rhythm disruption. In a study of 7,000 women, those who worked shift shifts were almost 50% more likely to experience an increase in RDW compared to women who worked day shifts. [R]
Bleeding
Severe and moderate injuries with heavy bleeding increase RDW. [R] Bleeding may not be visible, as is the case with intestinal and gastric bleeding. [r, r]
Blood transfusion
If a person undergoes multiple blood transfusions, their RDW may increase due to differences in blood composition between the donor and recipient. [r, r]
Liver disease
Increases in RDW occur in a variety of liver diseases, including hepatitis, alcoholic cirrhosis, biliary cirrhosis, and liver cancer. [R]
An observational study of 423 adults with liver disease found that their RDW was significantly higher than that of healthy controls. [R]
In another study of 446 hepatitis B patients, increasing RDW levels corresponded with increased liver size (hepatomegaly) and increased inflammation. [R]
Kidney disease
One of the kidney hormones, erythropoietin, is needed for the maturation of blood cells. Problems with the production of this hormone occur with kidney disease, leading to the development of RDW. [R] People with reduced kidney function have higher RDW levels. [R]
Alcoholism
Alcoholics can exhibit high RDW values without liver disease. This is because alcohol can have a toxic effect on red blood cells. [R]
Thalassemia
Thalassemia may cause increased RDW values. However, patients with thalassemia may also demonstrate normal RDW levels. [r, r, r]
Sickle cell anemia and hereditary spherocytosis
Sickle cell anemia is an inherited disease. People with this disease have higher RDW values because many of their red blood cells are misshapen. [R]
Hereditary spherocytosis (Minkowski-Choffard disease), another disease in which red blood cells become misshapen, also causes increased RDW levels. [r, r]
DISEASES IN WHICH RDW LEVELS INCREASE (https://medcraveonline.com)
Cancer
RDW rates are often higher in a variety of cancers, including stomach cancer, liver cancer, colon cancer, and kidney cancer. [r, r, r, r]
There are many factors in cancer that can interfere with the normal production of blood cells, including chronic inflammation and poor nutrition.
In cancer, RDW often increases with disease severity and metastasis. [R]
In a study of 25,000 people, the risk of cancer was 30% higher in those people who showed the highest RDW values compared to people with the lowest values. Postmenopausal women with the highest RDW values had a 22% increased risk of developing cancer. But no association was found between RDW values and cancer in premenopausal women. [R]
Cardiovascular diseases
According to a meta-analysis, an increase in RDW levels accompanies various cardiovascular diseases: acute coronary syndrome (including myocardial infarction), coronary heart disease, peripheral arterial disease, arterial hypertension, and also with atrial fibrillation. Higher RDW values predict more negative outcomes for these diseases.
Increased RDW has been associated with various types of cardiovascular disease in studies. [r, r, r]
In a study of 25,500 adults, each 1% increase in RDW resulted in a 13% increase in heart attack risk. Those people who showed low RDW values had a 71% reduced risk of having a heart attack (myocardial infarction) compared to people with the highest RDW levels. [R]
Elevated levels of RDW are associated with a high risk of cholesterol plaque building up in the arteries (atherosclerosis) in patients with hypertension. [R]
RWD is associated with autoimmune diseases
There is an association between high RDW levels and increased disease activity in autoimmune problems such as rheumatoid arthritis, lupus, psoriasis, Crohn's disease, Sjögren's syndrome, systemic scleroderma, and ankylosing spondylitis (ankylosing spondylitis). [r, r, r, r, r, r, r]
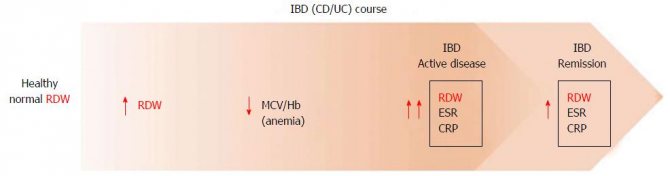
INCREASING RDW WITH INCREASING CROHN'S DISEASE/ULCERATIVE COLITIS ACTIVITY (https://www.wjgnet.com)
RWD and metabolic syndrome
People with higher levels of RDW show more advanced degrees of metabolic syndrome. This was found in studies involving more than 217,000 people. [r, r]
RWD and diabetes risk
In a study that monitored more than 2,600 people with normal blood glucose levels over 4 years, high RDW values increased the risk of developing diabetes by nearly 2 times compared to people with low RDW. [R]
RWD and risk of dementia (dementia)
In a study of approximately 2,500 older adults, higher RDW values had an increased risk of dementia. This risk was significant in those people who were not anemic. [R]
RWD is associated with mortality
High RDW values increase inflammation and oxidative stress, which contribute to the risk of mortality. In various studies, adult (45+) hospital patients with elevated RDW levels demonstrated a higher risk of cardiovascular mortality, infection, and all-cause mortality. [r, r, r]
Additionally, in a review of 13 studies (involving 10,410 patients), low RDW was associated with a lower risk of mortality. [R]
RDW and depression
The study, which followed 43,226 patients with depression for 5.3 years, measured RDW values at the time of diagnosis and in subsequent contacts with doctors. It was found that patients with cardiovascular diseases with increasing RDW had more advanced depressive syndromes.
What do abnormalities in women indicate?
The hemogram analysis may reflect an increased level of immune cells if women have one of these diseases:
- viral hepatitis A;
- acute infectious disease of the respiratory tract;
- viral disease with a high level of susceptibility (measles);
- a viral disease manifested in a rash (rubella);
- a bacterial infection that results in coughing fits.
The normal number of immune cells may be shifted upward if a woman suffers from an endocrine disease, hypothyroidism or thyrotoxicosis.
The level of lymphocytosis can be increased in cases of cancer and metabolic disorders in the body.
Decoding the quantitative indicator of immune cells will be completely different if few of them are identified.
Video:
In this case, women can be diagnosed with tuberculosis, which affects small areas of the respiratory system.
For this reason, toxic substances enter the blood, and the body is in a state of severe stress.
A decrease in the level of lymphocytes is associated with the appearance of cancer in a woman - multiple myeloma.
Together with a decrease in the number of immune cells, this serious illness can lead to the detection of a large amount of protein in urine.
But this disease proceeds in a special way: its initial stage is characterized by an increased level of immune cells, but later (as the tumor grows) there are very few lymphocytes.
The normal content of immune cells is often disrupted due to the occurrence of radiation sickness.
Since the maturation process of blood cells is disorganized, the body stops fighting germs and viruses. This disease can occur in an acute form if the exposure was strong and one-time.
The disease becomes chronic if irradiation is periodic, but its doses are small.
Decreased levels of immune cells may be caused by bone marrow dysfunction. At the same time, it loses the ability to produce the required volume of blood cells and becomes connective tissue.
Video:
For this reason, the blood has a low amount of all formed elements. Also, immune cells die during HIV infection.
When the norm of lymphocyte content is violated, it is recommended to undergo a comprehensive examination. After additional tests, the doctor will know what kind of disease the patient has.
Based on the data obtained, the appropriate treatment will be selected.
Decoding the results
The interpretation of the analysis is carried out only by a doctor. Having noticed an mcv value that is outside the normal range in the results, the specialist must determine the reasons for such a violation. For this purpose, additional diagnostics are carried out, which includes a survey and study of the patient’s medical history.
It is important to find factors in a person’s life that provoke a decrease or increase in the volume of red blood cells
If diagnostics reveals the presence of a disease, efforts must be directed toward its treatment. The medications that will be used in this case, affecting a specific problem, will help restore the required volume of red blood cells. There are no medications that can simply affect the mcv value in the blood, and taking them would be inappropriate, since the deviation of this indicator itself is not a disease
It is important to understand what exactly provokes its change
If the reason for the violation of the norm of red blood cells is an incorrect lifestyle or the consequences of treating a serious disease with antibiotics, the patient’s efforts must be directed to restoring the body. Healthy sleep, moderate exercise, proper nutrition and taking vitamin complexes will help restore the desired shape and normal value of red blood cells.
It is important to get advice from a qualified specialist and not to neglect the problem, so as not to treat its complications later. Normal red blood cells, called normocytes, are round, flat cells that are concave on both sides
This shape allows for maximum diffusion surface area while maintaining volume and can easily pass through narrow curved sections of the circulatory system. The MCV indicator in the blood (abbreviation for English mean cell volume, which means “average cell volume”) determines the average volume of a red blood cell
Normal red blood cells, called normocytes, are round, flat cells that are concave on both sides. This shape allows for maximum diffusion surface area while maintaining volume and can easily pass through narrow curved sections of the circulatory system. The MCV indicator in the blood (abbreviation for English mean cell volume, which means “average cell volume”) determines the average volume of a red blood cell.
If the average volume of erythrocytes is normal, the development of normocytic anemia is assumed, it occurs:
- hemolytic;
- aplastic;
- hemorrhagic;
- hepatic;
- endocrine.
High rate
When red cells are abundant, this indicates that the patient is developing macrocytic anemia.
The occurrence of this problem can be due to various reasons:
- lack of microelements (B12);
- lack of folic acid;
- megaloblastic anemia;
- presence of oncological education;
- hypothyroidism;
- malabsorption in the intestine;
- liver problems;
- myxedema;
- problems with the pancreas;
- diseased bone marrow with high leukocytosis;
- drug poisoning;
- alcohol toxicosis.
Frequent bleeding leads to a high index.
In some cases, macrocytosis occurs after long-term use of antidepressants. However, a clear connection with this fact has not been established.
The first signs of high erythrocytosis are blush on the face, redness of the skin on the body, headaches, and dizziness.
Low values
When the mcv value is low, this indicates the presence of microcytic anemia, which is a consequence of:
- chronic diseases and infections;
- iron deficiency;
- development of malignant tumors;
- lead poisoning;
- low hemoglobin levels;
- hereditary anemia;
- taking certain medications.
MCV less than normal is recorded with hypochromic anemia, microcytosis, or decreased hemoglobin synthesis. The latter directly affects the shape and fullness of red cells.
If there is less hemoglobin present than necessary, the red blood cells show less volume. Its synthesis also decreases when a person is sick with a genetic blood disease - thalassemia.
If someone experiences weakness, fatigue, tinnitus, absent-mindedness, severe pallor of the skin and memory impairment, he should consult a doctor. The number of red blood cells or their volume may have decreased.
Cell Variability
A person may show more than just an increase or decrease in MCV. In some cases, anisocytosis is diagnosed.
With this pathology, a microscope reveals many cells of different sizes, causing the blood to become too thick. The MCV indicator is closely related to another indicator, such as RDW, which characterizes the variability of cells in size.
Clinical and diagnostic significance of the relationship between RDW and MCV
In the diagnosis of diseases, changes in the ratio of MCV and RDW indicators are of great importance.
MCV high, RDW normal:
- chronic liver diseases;
- myelodysplasia.
MCV high, RDW high:
- B12 deficiency anemia;
- cold agglutination;
- hemolytic anemia;
- condition after chemotherapy.
MCV normal, RDW normal:
- norm;
- aplastic anemia.
MCV normal, RDW high:
- blood transfusion;
- initial stage of iron deficiency anemia;
- deficiency of vitamin B12 and/or folic acid;
- homozygous hemoglobinopathy;
- sideroblastic anemia;
- myelofibrosis.
Many diseases are accompanied by significant changes in the size and volume of red blood cells, so RDW is defined as a universal marker and precursor of some diseases.
MCV low, RDW normal:
- thalassemia;
- malignant neoplasms;
- hemorrhage;
- post-traumatic splenectomy;
- condition after chemotherapy;
- condition after blood transfusion.
MCV low, RDW high:
- iron deficiency;
- β-thalassemia;
- presence of hemoglobin H in the blood;
- erythrocyte fragmentation.
A decrease in RDW is observed very rarely and requires clarification of the meaning of other erythrocyte indices.

In sickle cell anemia, the MCV indicator may be unreliable, so the joint determination of RDW and MCV is of great diagnostic importance
Thus, for the differentiation of different types of anemia, the joint determination of RDW and MCV plays an important role. It should be taken into account that if there are a large number of abnormally shaped red blood cells in the blood, the MCV result may be unreliable (for example, red blood cells undergo severe deformation in sickle cell anemia or poikilocytosis). Even with severe anisocytosis, the content of MCV in blood cells may be normal, without reflecting the seriousness of the clinical situation.
Often the RDW value does not correspond to a decrease in MCV, which is a diagnostic error that is observed when visually counting cells under a microscope. In such a situation, it is recommended to repeat the analysis, and if the level is low again, then it is necessary to begin searching for the reason for the deviation from the norm.
How is the research going?
In modern medicine, equipment plays an important role in treatment. the same can be said about a blood test. On an empty stomach, blood is drawn either from a vein in the elbow or from a finger (this method is especially often practiced in the case of children), and then all the work is transferred to a modern analyzer, which conducts research quickly and with high quality, giving an accurate result .
It counts the number of red blood cells of different sizes per microliter of blood, calculates the average cell size and determines the degree of deviation from the norm of this indicator. The largest and smallest cells are also measured and the difference between this spread and the possible norm is analyzed. This indicator is recorded in femtoliters.
Of course, the equipment may not always be accurate; maximum accuracy of results can only be obtained by manual counting, but this is a very long and labor-intensive process, which is practically not used in modern medicine.
If deviations in this indicator occur, the blood test is performed again to obtain a reliable result, because the diagnosis cannot be made as a result of a single blood sample.
Preparation for the procedure
Since taking blood for a general analysis does not imply anything unusual, and the study itself is carried out regularly for almost all people, preparation does not require a person to take any special measures, but no one has canceled the standard recommendations before taking tests so that the results are reliable and correctly reflect the clinical picture:
RDW test is taken in the morning and on an empty stomach
Dinner in the evening of the previous day before donating blood should be light and at least 8 hours should pass between the last meal and the test, and preferably 12. It is highly not recommended to drink alcohol 2 days before the test, as it can significantly distort the results. Preferable 2 days before giving up fatty and fried foods, which have a negative impact on the body. Do not take a blood test after physiological and x-ray procedures. One hour before taking blood, it is recommended to refrain from smoking. It is advisable to exclude any physical and emotional stress; a 15-minute period is required before the test. respite and complete peace of mind Particular attention must be paid to the medications you are taking. Almost any medicine can distort the results of a blood test, so before donating blood you need to consult with a specialist: you may have to stop taking the medicine for a while to get an accurate clinical picture, or simply take the drug after the test.
If a repeat blood test is prescribed, it must be taken at the same time (since the composition of the blood may depend on the body’s circadian rhythms) and in the same laboratory. This is due to the fact that units and methods of measurement may vary between laboratories. Only if all recommended measures are followed will the result of the study be correct.
Blood test in Medart
The medical laboratory is equipped with modern high-precision equipment, high-quality reagents, all necessary consumables and qualified personnel. Our clients can rest assured of the reliability: if all preparation recommendations are followed, the results obtained will be 100% accurate.
Our team performs the work quickly, efficiently and with due understanding. Since there are people who are catastrophically afraid of any medical intervention, including blood sampling, we try to provide all our clients with the most comfortable and calm atmosphere, while performing all hematological studies at the highest level and providing accurate results.
With us, you can take a general blood test in a calm and comfortable environment and get a reliable result in the shortest possible time at an affordable price, without waiting in line for long hours, and then endlessly visiting doctors in an attempt to find out the result. We care about each of our clients and strive to do our work with the highest quality possible.
admin 02.12.2019
Decoding RDW in a blood test: the norm in women and men
There are two types of indicator:
- RDW-CV: reflects the percentage distribution of red blood cells by volume;
- RDW-SD: shows their standard deviation from the norm.
The RDW-CV norm in a clinical (general) blood test is the same for women and men. It is 11–15% and depends on the MCV indicator, changing which may increase the RDW. In children, for example in infants, due to the presence of fetal hemoglobin in the blood, physiological anisocytosis is observed, so the RDW indicator may be reduced. And only from 3 months does fetal hemoglobin begin to be replaced by adult hemoglobin.
The interpretation of the RDW-SD blood test shows the heterogeneity of cells in size and volume. This indicator does not depend on MCV and is measured in femtoliters (fl). The RDW-SD norm is 42 ± 5 fl.
If there are a small number of macrocytes and microcytes in the blood, the RDW-SD indicator will be as accurate as possible. The sensitivity of the RDW-CV indicator is slightly lower, but it most accurately reflects overall changes in red blood cell size.
Indications for RDW analysis
The RDW study is not prescribed separately. The indicator is part of the general blood test. It is examined if the following diseases are suspected:
- chronic inflammation of an infectious or autoimmune nature;
- acute and chronic liver diseases - hepatitis, cirrhosis;
- renal failure;
- heart diseases;
- oncological diseases;
- dysfunction of the brain.
RDW is a nonspecific indicator; it changes in various diseases.
In what cases is analysis prescribed?
The list of indications for a blood test for MVC is as follows:
Acute infections. In this case, analysis is necessary because the normal water-salt balance is disrupted. Accordingly, following this, the average volume of red blood cells gradually increases (you need to more actively transport oxygen).
And this is against the background of a decrease in the amount of fluid and sodium, potassium, and calcium. Those substances that indirectly help cellular respiration and nutrition.
- Anemia of various types. From classic, iron deficiency to more complex and dangerous forms. For example, megaloblastic or hemolytic. There are several options. In any case, red blood cells are transformed to ensure the normal functioning of the body.
- Violations of local and general immunity. The analysis is carried out without fail, because it is quite possible that the cause of frequent illnesses is a disruption of the hematopoietic system.
Despite the increase in the size of the red blood cell, more oxygen does not reach the tissues. Moreover, the maturation of defective cells takes longer. Hence the decline in the “performance” of the body’s defenses.
Diabetes. An extremely dangerous disorder that leads to generalized problems. Including in the hematopoietic system. The reason is the negative effect of glucose.
It does not transform and does not decay with the release of energy. On the contrary, it circulates throughout the body unchanged and harms the bone marrow. The study is prescribed among others. You also need to evaluate your sugar level.
Unstable hormonal levels. Specific substances of the body act as a kind of regulators of all vital processes. If they are produced too little or too much, the body does not work properly. Due to incorrect signals, problems with hematopoiesis begin.
Attention:
Meanwhile, hormonal imbalances can be caused by drugs. Conditioned by taking medications. The reason needs to be clarified separately. Under the supervision of an endocrinologist.
There are other reasons for ordering analysis. For example, unexplained weight gain. Or metabolic abnormalities. Exercise tolerance disorders and others.
At the discretion of the doctor, he orders the test in many cases. The list is approximate.
Decreased RDW in the blood
If the RDW level in the blood is reduced, then the red blood cells are too similar. This happens rarely; with violations, the dispersion in size increases much more often. If the erythrocyte distribution width is too small, the first step is to retake the analysis.
If the RDW remains low when the test is repeated, there are several options. Perhaps the total number of cells has become smaller and the size has become larger. This happens to pregnant women when hemoglobin F - fetal hemoglobin - appears in the blood. Another possibility is the appearance of a huge number of extremely small red blood cells. However, the frequency of such an event is extremely low. Other tests can help determine the exact cause of the decrease in RDW.
In addition, the reasons for the decrease in RDW relative to the norm are:
- improper absorption of vitamins and nutrients due to disruption of digestive processes, and as a result, their insufficient quantity in the body;
- a decrease in the amount of blood in the body due to injury, for physiological reasons (menstruation) or due to hidden internal bleeding (for example, an open stomach ulcer). In addition, the provision of blood through donation also provides characteristic indicators;
- surgical operations involving the removal of part of the tissue or organ;
- state of hormonal indicators. For example, red blood cell production may decrease in women at different points in the menstrual cycle and during pregnancy. Hormonal drugs can have the same effect on hematopoiesis.

Thus, the RDW parameter shows how unequal in size red blood cells are. Most often it is either normal or elevated. It is worth paying attention to the RDW parameter if you are concerned about fatigue, weakness and drowsiness, pallor, shortness of breath, since most often an increase in RDW is associated with anemia or blood transfusion.
Increase in RDW-CV in blood test
Conditions and diseases in which RDW-CV in a blood test is increased:
- iron deficiency;
- deficiency of vitamin B12 and folic acid;
- hemoglobinopathies;
- myelodysplastic syndrome;
- myelofibrosis;
- hemolytic crisis;
- cardiovascular pathology;
- red blood cell agglutination;
- leukocytosis above 50 x 109 cells/l;
- Alzheimer's disease;
- alcoholism;
- metastasis to the bone marrow;
- condition after surgery;
- condition after blood transfusion.
Normal levels can be determined in chronic diseases, heterozygous β-thalassemia, acute blood loss, hemolytic anemia outside of crisis.
RDW reduced
A low RDW value indicates that your red blood cells are uniform in size, which is desirable for health. [R] However, it is worth remembering that there is still a possibility of having some kind of disease. [R]
For example, with reduced RDW values, one may suspect disturbances in the functioning of the spleen, where damaged red blood cells are recycled. In addition, if RDW is low, it is worth thinking about the following possible reasons:
- Recent surgery
- Blood donation
- Severe blood loss (including hidden in the stomach and intestines)
- Hormonal disorders during pregnancy, puberty, and when taking contraceptives
Normal MCH values
The norm has different indications depending on the age of the person. The change can be influenced not only by age, but also by other multiple factors. Therefore, there are certain indicators for children and adults. Deviation in one direction or the other indicates serious pathological changes.
Norm for children by age
The data presented should not become a reason to do tests for your child. Before each fence, a small puncture is required, which is stressful for the child. Therefore, without strong indications for examination, this should not be done. Any stress leads to metabolic disorders and slow development. It may be short term, but it is a fact.
A change in the level of hemoglobin in the blood indicates the presence or absence of possible pathologies. The production of hemoglobin begins during the period of intrauterine development. Its level differs from the readings of an adult or an already born child. Complete replacement occurs during the first year of life.
What is MSI in blood test results?
Determining the level is quite simple by taking a general blood test
Important! To obtain reliable blood test data, samples are taken on an empty stomach before morning feeding. Two hours after breastfeeding, hemoglobin decreases. The test is usually prescribed by a doctor
The test is usually prescribed by a doctor.
But a mother can suspect a low level if she detects characteristic signs:
- pale skin;
- blue spots under the eyes;
- peeling of the skin.
The norm is:
- newborns – 170-240 g/l;
- the level in premature babies is slightly lower and amounts to 160-200 g/l;
- end of the first week of life – 160-200;
- further there is a slight increase, by the end of the first month of life, readings of 120-160 are considered the norm;
- by year – 120-140 and should remain this way for up to five years
Normal for teenagers
Puberty significantly affects hemoglobin level readings. Upon reaching 15 years of age, adolescents’ data are already equal to adults – 120-165 g/l. WHO (World Health Organization) does not consider deviations in indications to be a wide enough range. But it is desirable that it be within the specified limits.
Standards for adults
MCH in a blood test in adults has the following indicators:
| For women | 120-140 g/l |
| In men | 130-160 g/l |
In a pregnant woman, the level may differ, since her body provides hemoglobin for two. Sometimes their indicator is close to 110, which is not a violation. But the expectant mother must monitor the indications, since a deficiency leads to defective intrauterine development, fetal death or premature birth.
Important! The hemoglobin level in women can reach 90 m/g, which is associated with blood loss during menstruation. Lack of hemoglobin or anemia occurs in older people. This is due to age-related vitamin B12 deficiency. An insufficient amount of MCH is determined in alcoholics due to unsatisfactory synthesis of folic acid
An insufficient amount of MCH is determined in alcoholics due to unsatisfactory synthesis of folic acid.
Proper nutrition, the absence of bad habits and vitamin complexes will help to quickly restore the optimal amount. Lowering and raising the level are dangerous. Self-medication will not give the necessary improvement. A doctor's consultation and preliminary examination are necessary.
There are many foods that can normalize iron levels in the blood. Alcohol and smoking are destructive factors that can destroy all efforts
Normal RDW values
Normal RDW values are the same for men and women. The range of normal RDW in adults is 11.5 - 15.5%, but may vary slightly depending on the reagents used by different laboratories.
In newborn children, normal RDW values are increased to 14.9 - 18.7% due to stress at birth and adjustment to life outside the mother. But as children grow older, their normal RDW values gradually approach those of adults.
At the same time, with age, red blood cells become more varied in size (volume), which leads to an increase in RDW. [R]
How is the MCV blood test performed?
To determine the MCV level, you need to visit a laboratory that specializes in determining quality blood parameters, or take tests at a local clinic.
To obtain the most accurate diagnostic results with minimal risk of data errors, you will need to follow the rules for preparing for the donation of biological material, undergo the blood sampling procedure and wait for the test results.
Preparation
Includes the implementation of the following recommendations, which allow you to maintain the cellular composition of the blood at an optimal level without provoking its sudden changes.
The patient who will be tested will need to follow the following rules:
- 3 days before blood sampling, do not drink alcohol;
- take the test in the morning (preferably before 10-00);
- 2 days before diagnosis, exclude physical activity, do not engage in strength sports, do not lift heavy objects;
- have breakfast only after blood sampling, so that the stomach is empty (the best option would be to eat wheat, rice, pearl barley, barley porridge with vegetable salad).
It is recommended not to smoke 8 hours before donating blood. In the evening the day before the test, you should not overeat. All food consumed before laboratory testing should be light and not burden the digestive system.
Blood collection
A mandatory condition for submitting biological material for testing for MCV levels is taking blood on an empty stomach.
This procedure is performed using two methods, namely:
- ring finger bundle - pierced with an automatic pen with needles or a metal scarifier (about 1-2 ml of blood is taken by a laboratory assistant);
- ulnar vein - biological material is collected with a disposable syringe, which is filled with 5-10 ml of blood.
In order to obtain the most accurate research results, it is advisable to perform simultaneous collection of capillary and venous blood. This will allow for a comparative analysis of the selected samples, eliminating the possible occurrence of inaccuracies and errors in the operation of medical equipment.
How long to wait for answers
after delivery of biological material. In most cases, determining the average size of red blood cell units is only 1 of more than 20 parameters of the cellular composition of the blood that laboratory specialists need to determine.
If the staff of the clinic where the collected blood is tested uses automatic analyzers, the diagnostic process is significantly accelerated.
In laboratories that are not equipped with modern medical equipment and use microscopic research techniques, you will need to wait from 1 to 2 hours. In this case, the laboratory assistant performs an independent blood test, establishing the average volume of red blood cells using a microscope.

It is believed that the microscopic diagnostic method carries a greater number of errors, because there is a human factor involved. In order to save personal time and obtain the most accurate diagnostic results, it is recommended to donate blood in laboratories that are equipped with automatic analyzers.
What to do
Many pathologies that cause changes in the composition of the blood do not manifest themselves externally in the initial stages. This is why it is so important to have regular blood tests. Determining the RDW level will allow timely diagnosis of many diseases.
After receiving such test results, it is necessary to undergo additional examination. It will help determine why changes in blood composition are observed and what pathologies are causing this. Sometimes you can return normal blood counts by changing your diet, which will compensate for the lack of essential microelements. But most often, such disorders can be eliminated only after the underlying disease has been cured.
The essence of the study
The abbreviation MCV stands for mean corpuscular volume, and the analysis is based on measuring the volume of red blood cells (their diameter). In order to obtain accurate results, a verified amount of capillary or venous blood is taken. As a rule, this is half a test tube. Plus or minus.
The sample is then placed into the analyzer, which automatically calculates the final results.
Of course, MCV does not evaluate all red blood cells at once; this is impossible. But average values are always accurate and truly reflect the processes occurring in the patient’s body.
Upon completion, a research protocol is prepared. Among other things, doctors also reflect the average volume of red blood cells.
MCV in blood test is normal
The average volume of erythrocytes MCV, the norm in the analysis results is expressed in femtoliters (fl or fl). Less commonly, values are indicated in cubic micrometers (µm3). As studies of patients of different age groups show, the values of this parameter change with age. Taking into account this feature, the average volume of red blood cells, the norm of values is established for each age. In addition, the following factors may have some influence on MCV:
- eating before the study;
- consumption of alcoholic beverages;
- taking antidepressants.
In order to correctly interpret the analysis result and compare the value to the norm, only a specialist can evaluate the MCV. Children with increasing height and body weight experience a decrease in average red blood cell volume as they grow older. In addition to physiological changes in the indicator, there are also pathological ones associated with the development of the disease.

MCV blood test - interpretation, normal in children
In the first days after birth, the average volume of red blood cells in infants, MCV, is greater than in adults. As the baby develops and grows, the rate gradually decreases. A significant difference is noted closer to the child’s year of life. Only by the age of 16–18 is the indicator established at a level characteristic of healthy adults. The table shows how the average volume of red blood cells changes in children, the norm of this indicator.
| MCV norm in children, fl | |
| 0-1 day | Up to 128 |
| 1 Week | Up to 100 |
| 1 week-1 year | 77-79 |
| 1-2 years | 70-90 |
| 3-6 years | 76-90 |
| 7-12 years | 76-91 |
| 13-16 years old | 79-93 |
MCV blood test - interpretation, normal in men
Having figured out how MCV changes in a children's blood test and what this indicator is, let's look at the norms for men. Due to the physiological characteristics of the male body, greater muscle mass, the volume of circulating blood in men prevails over that of women. This explains the slightly lower average erythrocyte volume in men, since the indicator is the ratio of erythrocyte volume to blood volume. How MCV changes with age, the norm of the indicator - all this is shown in the table.
| MCV norm in men, fl | |
| 20-29 | 81-93 |
| 30-39 | 80-93 |
| 40-49 | 81-94 |
| 50-59 | 82-94 |
| 60-65 | 81-100 |
| over 65 years old | 78-103 |
MCV blood test - interpretation, normal in women
With the onset of puberty, ovulation occurs in a woman’s body every month. Moreover, if the egg is not fertilized, then after a few days it leaves the uterus along with the endometrium and blood. Heavy bleeding that lasts longer than normal provokes a decrease in circulating blood volume. This explains the situation when MCV in women exceeds that in men. How MCV changes in a blood test, the norm for women - all this is reflected in the table.
| MCV norm in women, fl | |
| 20-29 | 82-96 |
| 30-39 | 91-98 |
| 40-49 | 80-100 |
| 50-59 | 82-99 |
| 60-65 | 80-100 |
| over 65 years old | 80-99 |
Hemoleucograma
Blood hemoglobinReference values
Children
| Concentration | |
| 1st month | 135-165 g/l |
| 1st year | 110-140 g/l |
| 2-12 years | 119-155 g/l |
| Adults | |
| Men | 140-180 g/l |
| Women | 115-160 g/l |
Interpretation of the results obtained
Increase ↑ Hb
- Polycythemia;
- Erythrocytosis;
- Dehydration;
- Congenital or acquired cyanosis;
- Chronic heart and lung diseases;
- Renal cyst;
- Erythropoietin-producing tumors;
- Erythremia.
A false increase in results can be observed with hypertriglyceridemia due to serum turbidity, leukocytosis if the leukocyte count exceeds 25 x 109/l, the presence of HbC or HbS, easily precipitated globulins, for example, with myeloma or Waldenström's macroglobulinemia, progressive liver diseases, in heavy smokers due to formation of functionally inactive HbCO.
Decrease ↓ Hb
- Acute blood loss;
- Overhydration;
- Anemia.
Hematocrit
Reference values
| Men | 40-48% |
| Women | 36-42% |
Interpretation of the results obtained
Increase ↑ Ht
- Erythrocytosis: chronic lung diseases, altitude sickness, polycystic kidney disease, kidney tumors, accompanied by increased formation of erythropoietin;
- Condition of decreased volume of blood volume: peritonitis, burn disease;
- Dehydration: profuse diarrhea, uncontrollable vomiting, diabetes, excessive sweating.
Decrease ↓Ht
- Anemia;
- Pregnancy;
- Hyperproteinemia;
- Overhydration;
- A state of increased circulating plasma volume.
Red blood cells
Reference values
| Men | 4.0-5.1 x 1012/l |
| Women | 3.7-4.7 x 1012/l |
Interpretation of the results obtained
Increase ↑ Er
- Reactive erythrocytosis caused by oxygen deficiency in tissues (cor pulmonale; heart defects; emphysema) or caused by excessive formation of erythropoietins (polycystic kidney disease, neoplasms, Cushing's disease and syndrome);
- Dehydration;
- Decrease;
- Acute blood loss;
- Overhydration;
- Anemia.
Mean erythrocyte volume ( MCV ) MCV = Total volume of erythrocytes in a certain volume of blood / Number of erythrocytes in the same volume. The MCV value is expressed in femtoliters (1 fl = 1 µm3).
Reference values
| Age, gender | MCV, fl |
| < 2 weeks | 88 — 140 |
| 2-4 weeks | 91 — 112 |
| 4-9 weeks | 84 — 106 |
| 9 weeks – 4 months | 76 — 97 |
| 4 months - 5 years | 68 — 85 |
| 5 -10 years | 75 — 87 |
| 10 - 12 years | 76 — 94 |
| 12 – 18 years old | 73 — 98 |
| 18-65 years old | 80 — 100 |
| >> 65 years old | 81 — 103 |
Interpretation of the results obtained
Normal MCV levels can accompany the early stages of iron deficiency, sideroblastic and megaloblastic anemia, anemia in kidney diseases, endocrine disorders, acute posthemorrhagic anemia, hereditary microspherocytosis, anemia in leukemia, aplastic anemia, protein deficiency, mixed malnutrition. MCV less than normal values is assessed as microcytosis and is observed in iron deficiency anemia, thalassemia, sideroblastic anemia, anemia due to chronic infections, malignant tumors, systemic diseases, hemoglobinopathies. MCV greater than normal values is assessed as macrocytosis. Characteristic of megaloblastic, aplastic, severe hemolytic anemia, MDS, leukemia, during treatment with cytostatic drugs. The MCV index must be interpreted in conjunction with other blood parameters. A false decrease in MCV is observed with hyperglycemia (more than 20 mmol/l).
Hemoglobin content in an erythrocyte ( MCH ) MCH characterizes the average hemoglobin content in an individual erythrocyte, in picograms (pg). Based on the MCH value, hypo-, hyper- and normochromic anemias are distinguished. Clinical assessment of this indicator is carried out in conjunction with others.
Reference values
| Age, gender | MSN, pg |
| < 2 weeks | 30-37 |
| 2-4 weeks | 29-36 |
| 4-9 weeks | 27-34 |
| 9 weeks - 4 months | 25-32 |
| 4 months - 3 years | 24-30 |
| 3-15 years | 25-31 |
| Over 15 years old | 26-34 |
Interpretation of the results obtained
MCH within normal limits is observed in aplastic anemia, leukemia, MDS, anemia in kidney diseases, endocrine disorders, protein deficiency. A decrease is typical for severe iron deficiency anemia, thalassemia, sideroblastic anemia, anemia in malignant tumors, chronic infections, systemic diseases, etc. A high level of MCH is observed in megaloblastic anemia, MDS, leukemia, severe hemolytic anemia, and treatment with cytostatics.
Mean erythrocyte hemoglobin concentration (MCHC) MCHC is the number of grams of hemoglobin in 100 ml of erythrocytes (the ratio of weight to volume of erythrocytes). MCHC = HGB/HCT MCHC is the most stable indicator, because the maximum load of erythrocytes with hemoglobin is 36 g/100 ml with a normal cell volume.
Reference values
28-36 g/dl
Interpretation of the results obtained
A decrease in MCHC indicates a violation of hemoglobin synthesis and accompanies iron deficiency, sideroblastic anemia, thalassemia, polyetiological microcytic-hypochromic anemia in chronic infections, oncological and systemic diseases.
Red blood cell anisotropy coefficient (RDW)
Interpretation of the results obtained
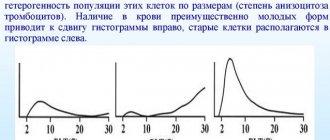
Reflects differences in red blood cell volume, i.e. degree of anisocytosis. This indicator provides a quantitative assessment of the dispersion of erythrocytes by volume, therefore RDV within the normal range (11.5-14.5%) indicates the presence in a given sample of only a population of erythrocytes homogeneous in volume (normo-, micro- or macrocytes). An RDW of more than 15.0% indicates the presence of cells heterogeneous in volume (micro-, normo-, macro- and schizocytes). In connection with the above, RDW should only be assessed in parallel with red blood cell histogram analysis and morphological examination of the blood smear. Red blood cell histogram is a graphical distribution of red blood cells by volume as a result of the analysis of several thousand particles with a volume from 40 fl to 240 fl. Red blood cell histograms clearly show the presence of microcytes, macrocytes or a mixed population of red blood cells, clearly demonstrating positive dynamics in the treatment of anemia. The pattern of the erythrocyte histogram may change if there are a large number of schizocytes, macrothrombocytes, erythrocyte or platelet agglutinates, and small lymphocytes in the blood being tested. A plateau to the right of the peak indicates the presence of significant amounts of red blood cell fragments, platelet macroforms, or platelet aggregates. An additional peak due to elements greater than 140 fL is most often associated with the presence of erythrocyte agglutinins. In chronic lymphocytic leukemia with a predominance of small lymphocytes, an additional peak appears in the erythrocyte histogram in the region of approximately 200 fL.
Reticulocytes The reticulocyte count reflects the rate of red blood cell production in the bone marrow. Their counting is important for assessing the degree of erythropoiesis activity. When erythropoiesis accelerates, the proportion of reticulocytes increases, and when it slows down, it decreases. In the case of increased destruction of red blood cells, the proportion of reticulocytes may exceed 50%. With sharply accelerated erythropoiesis, normoblasts (precursors of reticulocytes) may appear in the blood. Reticulocytes are found in greater numbers in newborns than in adults.
Reference values
| Age | Meaning, % |
| 0-2 days | 30-70 |
| 2-6 days | 10-30 |
| 6-8 days | 0-10 |
| 8 days - 5 weeks | 2-20 |
| 5 weeks - 7 weeks | 3-35 |
| 7 weeks - 10 weeks | 4-48 |
| 10 weeks - 12 weeks | 3-42 |
| 12 weeks - 15 weeks | 3-36 |
| 15 weeks - 12 months | 2-28 |
| 1-120 years old husband | 5,1-18,1 |
| 1-120 years old women | 5,0-17,0 |
It is advisable to use the “reticulocyte index” to assess the severity of anemia: % reticulocytes x hematocrit of the patient/45 x 1.85 where: 45 is a normal hematocrit, and 1.85 is the number of days required for the entry of new reticulocytes into the peripheral blood Index < 2 – evidence of a hypoproliferative component of anemia; index > 2-3 – evidence of increased red blood cell production
Interpretation of the results obtained
Increased ↑reticulocyte content
- Blood loss or destruction of red blood cells (3-6 times increase);
- Hemolytic anemia (up to 300%);
- Treatment of B12-deficiency anemia (reticulocyte crisis on days 5-8 of vitamin B12 therapy). The number of reticulocytes can increase up to 200%;
- Effective therapy of iron deficiency anemia with iron preparations (8-12 days of treatment);
- Thalassemia;
- Malaria;
- Other hematological diseases (polycythemia, cancer metastases to the bone marrow);
- Acute oxygen starvation.
Decreased ↓ reticulocyte content
- Aplastic anemia;
- Hypoplastic anemia;
- Untreated B12 deficiency anemia;
- Autoimmune diseases of the hematopoietic system;
- Alcoholism;
- Cancer metastases to bone;
- Myxedema;
- Kidney diseases.
A comprehensive interpretation of all red blood indicators provided by modern hematological analyzers provides rich information for diagnosing erythropoiesis disorders, monitoring therapy, and assessing the severity of pathology.
Leukocytes
Reference values
4.0-9.0 x 109/l
Interpretation of the results obtained
Increased ↑ leukocyte count
- Infections;
- Inflammatory conditions Leukemia and other neoplasms;
- Injuries;
- Uremia.
Decrease ↓ leukocyte count
- Toxic lesions or effects of ionizing radiation;
- Metastases to the bone marrow;
- Hypersplenism;
- Myelodysplastic syndrome;
- Sepsis;
- Anaphylactic shock;
- Collagenoses.
Leukocyte formula
Reference values
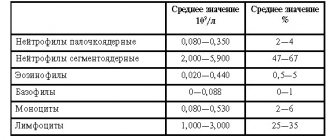
- Band neutrophils 1-5%
- Segmented neutrophils 40-70%
- Eosinophils 1-5%
- Lymphocytes 20-45%
- Basophils 0-1%
- Monocytes 3-8%
Interpretation of the results obtained
Shift to the left: (in the blood metamyelocytes, myelocytes)
- Acute infectious diseases;
- Acidosis and comatose diseases;
- Physical stress;
- Shift to the left with rejuvenation: (in the blood there are metamyelocytes, myelocytes, promyelocytes, myeloblasts, erythroblasts):
- Chronic leukemia: erythroleukemia, myelofibrosis;
- Metastases of malignant neoplasms;
- Acute leukemia.
Shift to the right: (hypersigmented granulocytes in the blood)
- Megaloblastic anemia;
- Kidney and liver diseases;
- Condition after blood transfusion.
Neutrophils
Interpretation of the results obtained
Neutrophilia
- Infections: bacterial, fungal, spirochetal, some viral, rickettsial, parasitic;
- Inflammatory process: rheumatism, rheumatoid arthritis, tissue damage (after surgery), ischemic necrosis, gout, hypersensitivity to drugs, smoking, colitis, pancreatitis, nephritis, myositis, thyroiditis, dermatitis, periodontitis;
- Intoxications: diabetes mellitus, uremia, eclampsia, necrosis of liver cells,
- Blood diseases: chronic myeloid leukemia, polycythemia vera, myelofibrosis with myeloid myeloplasia, thrombocytopenia, condition after splenectomy, hemolytic anemia, bleeding, chronic idiopathic leukocytosis, malignant tumors;
- Mental and emotional agitation;
- Drugs: corticotropin, corticosteroids, adrenaline, lithium, endotoxins, histamine, heparin, acetylcholine, insect poisons, lead, mercury, ethylene glycol, digitalis, carbon dioxide, turpentine, chlorpropamide.
Neutropenia
- Infections: bacterial, viral, rickettsial, protozoal, debilitating infections of any type, especially in elderly and weakened people;
- Blood diseases: aplastic anemia, acute leukemia, idiopathic neutropenia, hypersplenism, megaloblastic anemia, anemia due to decreased bone marrow function, iron deficiency anemia;
- Anaphylactic shock;
- Hypothyroidism;
- Thyrotoxicosis;
- Cirrhosis of the liver;
- Periodic neutropenia;
- The influence of drugs: painkillers, tranquilizers, cyclic antidepressants, sulfonamides, antithyroid drugs, anticonvulsants, antihistamines, antimicrobials, hypoglycemics, etc.
Eosinophils
Interpretation of the results obtained
Eosinophilia
- Allergic diseases;
- Skin diseases;
- Parasitic infestations;
- Blood diseases;
- Malignant tumors;
- Pulmonary infiltration;
- Irradiation;
- Periarteritis nodosa;
- Some poisonings;
- Idiopathic eosinophilia;
- Congenital eosinophilia;
- Effect of drugs: aminosalicylic acid, chlorpropamide, imipramine, penicillin, sulfonamides, etc.
Eosinopenia
- Most pyogenic infections;
- Childbirth, eclampsia;
- “aggressive” surgical interventions;
- Shock;
- Effect of drugs: corticotropin, adrenaline, glucocorticoids, nicotinic acid, nicotinamide.
Basophils
Interpretation of the results obtained
Basophilia
- Chronic myeloid leukemia;
- Polycythemia vera;
- Chicken pox;
- Hypersensitivity reaction to food;
- Nephrosis;
- Chronic hemolytic anemia;
- Ulcerative colitis;
- Lymphogranulomatosis;
- Condition after splenectomy;
- influence of medications: estrogens, antithyroid drugs, desipramine.
Basopenia
- Hyperthyroidism;
- Ovulation;
- Pregnancy;
- Stress;
- Acute infections;
- Cushing's syndrome.
Lymphocytes
Interpretation of the results obtained
Lymphocytosis
- Infectious mononucleosis;
- Infectious lymphocytosis;
- Infectious hepatitis;
- Whooping cough;
- Brucellosis;
- Tuberculosis,
- Syphilis;
- Acute and chronic lymphocytic leukemia;
- Heavy chain diseases;
- Effect of drugs: aminosalicylic acid, haloperidol, narcotic analgesics, phenytonin, lead poisoning, tetrachloroethane.
Lymphopenia
- Acute infections;
- Milliary tuberculosis;
- Loss of lymph through the intestines;
- Lymphogranulomatosis;
- Aplastic anemia;
- Kidney failure;
- Cancer;
- Immunodeficiency conditions;
- Effect of drugs: corticotropin, glucocorticoids, lithium, nicotinic acid.
Monocytes
Interpretation of the results obtained
Monocytosis
- Subacute septic endocarditis;
- Infections;
- Granulomatosis;
- Ulcerative colitis;
- Acute monocytic leukemia;
- Myelomonocytic leukemia;
- Multiple myeloma;
- Aplastic anemia;
- Collagenoses;
- The influence of drugs.
Monocytopenia
- Bone marrow damage;
- After treatment with glucocorticosteroids;
- For infections with neutropenia.
Platelets Diagnostic value Identification of causes of bleeding caused by thrombocytopenia and/or thrombocytopathy.
Reference values
The number of platelets in the blood is 180-320×109/l.
Interpretation of the results obtained
Platelet pathology is the cause of bleeding in almost 80% of cases. Thrombocytopenia is its most common manifestation. Physiological fluctuations in the number of platelets in the blood during the day are approximately 10%. In women during menstruation, the platelet count can decrease by 25-50%. Platelets perform angiotrophic, adhesive-aggregation functions, participate in coagulation processes, and ensure blood clot retraction. They are able to carry circulating immune complexes on their membrane and maintain vasospasm. In 80-85% of patients with hemorrhagic diathesis, disturbances in the hemostatic system are caused by a decrease in the number or functional activity of platelets. In cases where the platelet count is less than 150 × 109/L, thrombocytopenia should be noted. The frequency of this phenomenon is quite high - from 10 to 130 new cases per 1 million population. There are acute and chronic thrombocytopenia. The latter is diagnosed when its duration exceeds 6 months. In individuals with platelet levels above 50×109/L, thrombocytopenia is extremely rarely accompanied by bleeding. However, a decrease in platelets below 100×109/L can accompany serious pathology. In this regard, the cause of each case of thrombocytopenia must be clarified.
Decreased ↓ platelet count (<180x109/l)
- A decrease in the number of platelets in the blood is observed with inhibition of megakaryocytopoiesis, impaired platelet production, with splenomegaly, increased destruction and/or utilization of platelets. The following conditions and diseases may be the cause of a decrease in platelet count.
Thrombocytopenia associated with decreased platelet formation (hematopoietic insufficiency) Acquired
- Idiopathic hypoplasia of hematopoiesis;
- Viral infections (viral hepatitis, adenoviruses);
- Intoxication (ionizing radiation, myelosuppressive chemicals and drugs, some antibiotics, uremia, liver disease);
- Tumor diseases (acute leukemia, metastases of cancer and sarcoma to the bone marrow, myelofibrosis and osteomyelosclerosis);
- Megaloblastic anemia (deficiency of vitamin B12 and folic acid);
- Nocturnal paroxysmal hemoglobinuria.
Hereditary
- Fanconi syndrome;
- Wiskott-Aldrich syndrome;
- May-Hegglin anomaly;
- Bernard-Soulier syndrome.
Thrombocytopenia caused by increased platelet destruction Autoimmune idiopathic
- Werlhof's disease
Secondary
- with systemic lupus erythematosus;
- viral infection;
- chronic lymphocytic leukemia, etc.;
- in newborns due to the penetration of maternal autoantibodies into the internal environment of the child’s body.
Isoimmune
- neonatal;
- post-transfusion.
Hapten drugs (hypersensitivity to certain drugs). Associated with mechanical damage to platelets:
- for heart valve replacement;
- extracorporeal circulation;
- with nocturnal paroxysmal hemoglobinuria (Marchiafava-Micheli disease).
Thrombocytopenia caused by platelet sequestration, sequestration in hemangioma, sequestration and destruction in the spleen:
- hypersplenism – Gaucher disease;
- Felty's syndrome;
- sarcoidosis;
- lymphoma;
- splenic tuberculosis;
- myeloproliferative diseases with splenomegaly, etc.
Thrombocytopenia associated with increased platelet consumption
- Disseminated intravascular coagulation syndrome;
- Thrombotic thrombocytopenic purpura, etc.
Increased ↑ platelet (>320*109/l)
- An increase in the number of platelets in the blood (thrombocytosis) may be primary, i.e. be the result of primary proliferation of megakaryocytes, and secondary, reactive, occurring against the background of any disease.
An increased number of platelets can cause the following diseases: Primary thrombocytosis
- essential thrombocythemia (the number of platelets can increase to (2000-4000)x109/l or more);
- erythremia;
- chronic megakaryocytic myeloid leukemia and myelofibrosis.
Secondary thrombocytosis:
- acute rheumatism;
- rheumatoid arthritis;
- tuberculosis;
- cirrhosis of the liver;
- ulcerative colitis;
- osteomyelitis;
- amyloidosis;
- carcinoma;
- lymphogranulomatosis;
- lymphoma;
- condition after splenectomy (for 2 months or more);
- acute hemolysis;
- 7-10 days after the onset of subacute toxic-infectious DIC syndrome;
- after acute bleeding;
- for malignant neoplasms (a precursor to a tumor of the lung, pancreas);
- chronic DIC syndrome.
Mean platelet volume (MPV)
Reference values
7.4 – 10.4 fl
Interpretation of the results obtained
In apparently healthy individuals, MPV is inversely related to the platelet count. MPV increases with age: from 8.6 - 8.9 fL in children 1-3 years old to 9.3-10.6 fL in people over 70 years of age.
Increase ↑ MPV
- Idiopathic thrombocytopenic purpura;
- Thyrotoxicosis;
- Diabetes;
- Atherosclerosis;
- Myeloproliferative diseases;
- Macrocytic thrombocytodystrophy of Bernard-Soulier;
- May-Hegglin anomaly;
- Posthemorrhagic anemia;
- Smokers and alcoholics.
Decrease ↓ MPV
- Condition after splenectomy;
- Wiskott-Aldrich syndrome.
Platelet distribution width (PDW) PDW – platelet distribution width – quantitatively reflects the heterogeneity of the population of these cells in size (degree of platelet anisocytosis). This indicator changes in myeloproliferative diseases.
Reference values
15,0 – 17,0%.
Graphic distribution of platelets by size (histogram) Modern hematological analyzers draw thrombocytometric curves (histograms of platelet distribution by volume). There is a connection between the size of platelets and their functional activity, the content of biologically active substances in platelet granules, the tendency of cells to adhere, and changes in platelet volume before aggregation. The presence of predominantly young forms of platelets in the blood leads to a shift of the histogram to the right, old cells are located in the histogram on the left. Consequently, as platelets age, their volume decreases.