To verify an oncological diagnosis, it is recommended in all cases to perform a biopsy - intravital removal of material in the form of a piece of tissue from an area in which the presence of a benign or malignant tumor is suspected for the purpose of its subsequent morphological assessment. A biopsy allows not only to confirm or exclude the presence of oncology, but also to recognize the histological type of tumor, which is key to determining further treatment tactics and prognosis.
- Indications for gastric biopsy
- Contraindications to gastric biopsy
- Preparation for the procedure
- Biopsy sampling methods
- Procedure
- How the material is examined
- Possible complications and consequences of a biopsy
Gastric biopsy is widely used in gastroenterology. It is carried out not only to identify tumors, but also to diagnose other non-tumor diseases. The study is prescribed in combination with esophagogastroduodenoscopy, during which the condition of the mucosa can be assessed and a biopsy specimen taken for histological examination. Previously, gastric biopsy was performed “blindly”, through a gastric tube, but with the introduction of endoscopy, it became possible to accurately take a tissue sample with minimal damage to the mucosa.
Indications for gastric biopsy
Endoscopic examination of the stomach with biopsy sampling is indicated in the following cases:
- Any neoplasms of a tumor nature.
- Sluggish and long-term non-healing ulcers of the mucous membrane.
- Gastritis that is difficult to treat.
- Gastritis with an unclear type of secretion.
- Stomach ulcer.
- Visually detectable changes in the mucous membrane (suspicion of intestinal metaplasia).
- A combination of dyspeptic symptoms and unmotivated weight loss, especially in people with a family history of cancer.
- The presence of polyps of the mucous membrane.
- Previous surgical interventions on the stomach for diagnosed cancer.
Performing a gastric biopsy can serve several purposes:
- Study of the morphological structure of the affected area (differentiation between benign and malignant processes is carried out).
- Determination of inflammatory activity.
- Determination of the type of mucosal epithelial dysplasia.
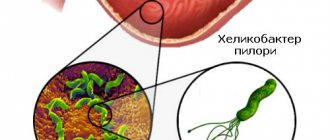
- Detection of Helicobacter pylori.
- Monitoring the effectiveness of treatment carried out after the diagnosis of stomach cancer.
Stomach
Stomach tumors may appear as ulcers, polyps, submucosal formations, or thickened folds of the mucous membrane. Adequate sampling of material sometimes requires the use of combined techniques. Punch biopsy gives the best results for ulcerative or polypoid formations. Several pieces should be taken from the edge of each quadrant of the ulcer and its bottom. The combination with brush cytology increases the possibilities of morphological diagnosis. Biopsies must be taken from all small polyp-like formations; polyps larger than 2 cm, if technically possible, must be removed entirely. Removal of gastric polyps is associated with a higher risk of bleeding than removal of intestinal polyps, so the possibility of prescribing antisecretory therapy in the postoperative period should be considered.
Endoscopic mucosal resection is used to remove material from thickened folds of the gastric mucosa in order to exclude gastric cancer and to treat its early forms. This method removes foci of early gastric cancer less than 20 mm in size that do not extend beyond the mucous membrane, which is confirmed by endoscopic ultrasound or based on endoscopic criteria. The pathological focus is raised above the submucosal layer by endoscopic injection of fluid, and then resected using one of the technical techniques.
In patients with peptic ulcer disease, maltoma and in persons with an increased risk of developing stomach cancer (gastric cancer in relatives according to anamnestic data), the presence of Hp infection should be excluded or confirmed. For this purpose, methods are used based on the study of a biopsy obtained during endoscopy. This includes testing for urease activity (rapid urease test), identification of typical convoluted bacteria by histological examination, and isolation of bacteria in culture. In untreated patients, material should be collected from the lesser curvature of the antrum near the angle of the stomach. The rapid urease test is inexpensive, highly specific and can be performed in an endoscopy department, giving results within 1 hour. If the urease test is negative, other methods for detecting HP can be used.
Histological examination of a gastric biopsy should include assessment of inflammatory cell infiltration and the presence of typical tortuous bacteria, which may require additional staining techniques. The presence of pronounced inflammatory cell infiltration in the absence of bacteria requires a serological test (determination of Hp-specific antibodies), a urease breath test, or detection of antigen in feces. Culture testing is designed to detect antibiotic resistance, but has low sensitivity and is difficult to perform.
The sensitivity of methods for detecting Hp in tissue samples may be reduced in patients receiving proton pump inhibitors or antibiotics, in those who have recently received anti-Helicobacter therapy (but the infection persists), or in the presence of gastrointestinal bleeding. In such patients, material should be collected from many areas of the mucous membrane of the antrum and body of the stomach, and a negative rapid urease test should be supplemented by other diagnostic methods. If possible, patients should be asked to stop taking proton pump inhibitors one week before testing for Hp.
Contraindications to gastric biopsy
Gastric biopsy has a number of contraindications, both absolute and relative. The first group includes:
- Acute somatic pathologies requiring emergency medical care (stroke, myocardial infarction, bronchial asthma attack).
- Cicatricial narrowing of the lumen of the esophagus, making it impossible to advance the endoscope.
- Aortic aneurysm.
Relative contraindications for gastric biopsy include the following conditions:
- Inflammatory process in the nasopharynx.
- Feverish condition.
- Epilepsy.
- Blood clotting disorders, hemorrhagic diathesis.
- Mental illnesses in the acute stage.
- Heart failure and hypertensive crisis.
Symptoms
Oncology is not detected at an early stage, as it does not cause any specific symptoms. Below are the symptoms of stomach cancer.
- Indigestion or heartburn
- Pain and discomfort in the abdominal area
- Nausea and vomiting, particularly vomiting solid food soon after eating
- Diarrhea or constipation
- Bloating after eating
- Loss of appetite
- Feeling like food is stuck in the throat while eating
Symptoms of advanced cancer include:
- Weakness and fatigue
- Bloody vomiting and blood in stool
- Unexplained weight loss
It is important to remember that complaints can also be caused by many other diseases, in particular a stomach virus or ulcer.
Preparation for the procedure
No specific preparation is required for the biopsy. It is enough to follow the general rules shown before performing gastroscopy. First, the doctor explains to the patient the purpose and course of the procedure and obtains his consent. In case of emotional lability, before endoscopic examination of the gastric mucosa and taking a biopsy, mild sedatives may be prescribed to calm the patient. In addition, it is necessary to carefully collect anamnesis to identify allergic reactions to drugs used during endoscopy with biopsy (especially anesthetics).
It is recommended to exclude hot and spicy foods and alcohol from the diet a week before the examination, as they can irritate the mucous membranes and distort the picture. You should also reduce your consumption of foods that cause increased gas formation. You should not eat food 6 hours before the procedure, drink 2 hours before. In some cases, it is recommended to rinse the stomach immediately before the biopsy. For example, with pyloric stenosis, the evacuation of food from the stomach into the duodenum may be slowed down.

How is a biopsy taken?
Taking a biopsy during endoscopy is an optional procedure. Sometimes, during a routine examination or diagnosis of an unclear disease, the decision is made by the endoscopist if he notices a pathological focus or suspects its presence. Taking a biopsy during FGDS is necessary to clarify the nature of the disease. No special preparation is required; the patient is prepared for endoscopy (FGS, colonoscopy), which is performed under anesthesia or sedation.
The patient is placed on his side, after anesthesia, an endoscope is inserted, the diagnostician examines the walls of the organs, and if necessary, takes biomaterial. Taking a biopsy during endoscopy lasts a few seconds and does not lengthen the procedure; it is absolutely painless. Upon completion, the patient remains under observation for 1-2 hours, then he can go home.
Biopsy sampling methods
A tissue sample from the gastric mucosa can be obtained by two methods. The first method is surgical. It is carried out directly during an operation on an organ, when the question arises about the volume of tissue to be removed. A small section of tissue is removed with a scalpel and sent urgently to the laboratory. The doctor examines the drug under a microscope and makes a conclusion after 10 - 15 minutes. During this time, the operating team does not perform any actions. After deciphering the biopsy, the operation resumes and the necessary adjustments are made to the extent of the surgical intervention.
The more common method is endoscopic. For this purpose, a flexible probe is used - a fiberscope, at one end of which there is a camera lens, an LED flashlight, holes for air and water supply, and a mount for attachments. At the other end of the tube there is a handle with a control unit and an eyepiece. Nowadays, targeted biopsy is mainly used because it minimizes the risks of the procedure.
What is a biopsy?
For examination under a microscope, a small amount of tissue, a few millimeters in size, is sufficient. It is treated with special reagents, impregnated with paraffin, cut with a microtome (a device that makes extremely thin sections) and examined under high magnification. Different types of staining are needed to see microorganisms, an anomaly in the differentiation of cellular structures inherent in tumors. This takes time, so it will take about two weeks to see results.
Usually, at least 3 pieces are taken from different places in each suspicious area; in addition, a separate biopsy specimen is required to determine Helicobacter; it is treated with a special paint. The more material is taken, the higher the likelihood of identifying disorders and diagnosing pathology, because some samples may not contain pathologically altered objects. Therefore, the number of samples can be 10-15 pieces.
Biopsy can be needle, loop, or brush biopsy, but for fibroendoscopy, forceps is used. Using a micro-instrument (forceps) inserted through a flexible endoscope hose, the epithelium is pinched off and sent to the laboratory. The ability to monitor the procedure eliminates damage to large arteries and veins.
Procedure
A gastric biopsy can be performed on an outpatient basis, under local anesthesia: the pharynx and pharynx are irrigated with a 10% lidocaine solution to suppress the gag reflex. The subject should be in a lying position on his left side. The endoscope is inserted with gentle movements, and all areas of the mucous membrane along the esophagus and stomach are examined one by one. To improve visualization, air is injected, which straightens the folds of the hollow organ.
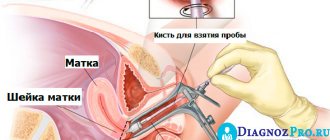
A piece of tissue is pinched off from the area of mucosa being examined with a special biopsy instrument (biopsy forceps) inserted into the instrument port of the fiberscope. To increase the accuracy of histological examination, material is collected from several points of the mucosa (at least 4), and the biopsy sample is taken from the border between the pathologically changed and normal areas.
An additional technique of chromatogastroscopy is also used, which simplifies the determination of the boundaries between different areas of the surface under study. A dye is sprayed over the gastric mucosa, which is unevenly absorbed (depending on the functional and organic state of the mucosa). For staining you can use Lugol's solution, methylene blue, Congo red. The area that is stained more intensely is most often pathologically changed, and the biopsy is performed on the periphery of this area (if there is an ulcer or tumor, then in the center too). The duration of the procedure can vary from 10 to 40 minutes and depends on the scope of the study.
After a gastric biopsy, it is advisable not to eat for 2 hours. After this period, you should avoid eating hot foods and drinks for some time. As a rule, there is no pain either during or after the procedure, but there may be slight discomfort in the epigastric region. In rare cases, there may be slight bleeding that stops on its own.
Contraindications
Complete contraindications to biopsy:
- serious condition of the patient with decompensation of the functional capabilities of the heart,
- inability to contact the patient due to severe mental pathology,
- Excessive bleeding due to a clotting disorder.
Temporary contraindication to diagnostic manipulation: exacerbation of inflammatory diseases and infectious diseases, including respiratory infections.
Specific “organ” contraindications also exist; they are relative, that is, they are neglected when absolutely necessary, which does not exclude the utmost caution when performing the diagnostic procedure:
- stricture of the esophagus with the impossibility of performing an endoscope,
- swelling of the nasal mucosa makes breathing difficult when the endoscope is inserted through the mouth,
- The esophageal wall, thinned by pathological changes, increases the likelihood of damage during manipulation.
How the material is examined
The piece of tissue taken during the biopsy is placed in an airtight container with a preservative. The container is signed (full name of the person being examined and the date of the procedure) and sent to the laboratory.
In the histological laboratory, the tissue is fixed in formalin and embedded in paraffin; if an urgent examination is performed, the tissue is frozen. Then the laboratory assistant uses a microtome to make thin sections of the tissue being examined. The specimen is then placed on a glass slide, stained, dried, and examined under a microscope.
After studying the drug, the pathologist issues a conclusion in which he indicates:
- thickness of the gastric mucosa;
- the nature of the epithelial tissue;
- the presence of dysplasia or metaplasia of the epithelium;
- degree and nature of inflammation;
- the presence of atypical cells, their maturity and location;
- presence of H. pylori, degree of contamination.
A possible additional analysis may be the polymerase chain reaction of a biopsy specimen, which gives the most accurate result in terms of diagnosing Helicobacter pylori.
Morphologically, the presence of the following signs speaks in favor of stomach cancer: abnormal cell shape (polymorphism not typical for this area), cell size (usually tumor cells are larger), size and fragmentation of nuclei, multinucleation, pathological inclusions in the cytoplasm.
The results of a gastric biopsy, if it is not urgent, are given to the patient and the attending physician 10 to 14 days after the procedure. An urgent study is performed on the same day, but its accuracy is somewhat inferior to a planned study.
Possible complications and consequences of a biopsy
With proper preparation and a biopsy performed by a qualified doctor using modern equipment, the risk of complications is significantly reduced. However, in practice the following situations may rarely occur:
- acute bleeding from the area where the material was taken;
- perforation of the gastric mucosa. It occurs extremely rarely, usually when a “blind” biopsy is performed by an inexperienced specialist);
- the occurrence of allergic reactions to the anesthetic;
- damage to teeth and oral mucosa.
In addition, after the procedure, long-term consequences may occur, which, as a rule, are facilitated by concomitant pathology, as well as some anatomical features:
- bleeding from a vessel damaged during biopsy;
- aspiration pneumonia due to violation of the technique of inserting and removing the fiber gastroscope or vomit entering the respiratory tract;
- inflammatory diseases of the upper digestive system.
A gastric biopsy is in most cases a painless and low-traumatic procedure, which, despite its relative simplicity, can provide a lot of important information about the nature and course of the pathological process.
Book a consultation 24 hours a day
+7+7+78
Cost and duration of the study
| Name | Term | Cost, rub. |
| Histology without immunohistochemistry | from 3 days | 12 500 |
| Histology with immunohistochemistry | from 3 days | 28 300 |
* Arrangement and payment for delivery of raw material (not in blocks) is carried out by the client.
For any questions you may have, you can consult our medical administrator by phone: 8-800-555-92-67 or write to us on WhatsApp: +7 925 740 05 87