Radioisotope examination of the thyroid gland - scintigraphy - is not a new and well-proven diagnostic method.
The principle of scintigraphy is to record the process of accumulation of a radiopharmaceutical (RP) by the tissues of the thyroid gland and visualize the response radiation using special equipment (gamma camera). Analysis of the obtained images of the thyroid gland makes it possible to study in detail the functionality of the organ as a whole and each of its parts separately, to identify pathological changes occurring in the gland and to assess the degree of their severity.
Based on the scintigraphy conclusion, the doctor plans a scheme for further treatment and/or rehabilitation of the patient.
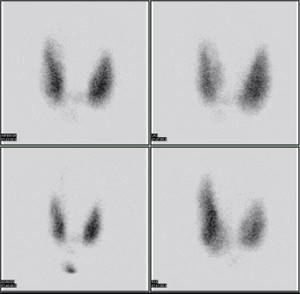
Photo: Myohan at en.wikipedia
Indications
The endocrinologist prescribes thyroid scintigraphy only if there are certain indications:
- anatomically incorrect location of the gland;
- congenital anomalies of the structure or development of the thyroid gland;
- thyrotoxicosis (differential diagnosis);
- “hot” (hyperfunctioning) and “cold” (non-functioning) nodes in the gland;
- suspicion of tumor formations.
Note: Thyrotoxicosis is a condition in which the thyroid gland intensively produces hormones; this is a symptom complex with
- diffuse toxic goiter,
- thyrotoxic adenoma of the thyroid gland (Plummer's disease),
- pituitary adenoma,
- subacute thyroiditis (de Quervain's disease),
- autoimmune thyroiditis,
- autoimmune ophthalmopathy,
- vegetative-vascular dystonia, etc.
Therefore, if thyrotoxicosis is suspected, it is necessary to carry out differential (comparative) diagnosis using scintigraphy.
Research result
Most often, this study is prescribed to identify nodes and correctly assess their activity. Scintigraphy can identify “cold” and “hot” zones. “Cold” nodes do not have the ability to accumulate radioisotopes, so this indicates a nodular goiter or a neoplasm. “Hot” nodes, on the contrary, accumulate radioisotopes, thereby producing hormones without the control of thyroid-stimulating hormone. In addition, scintigraphy allows you to evaluate other absorption parameters that indicate other thyroid diseases.
Methodology
Depending on the radiopharmaceutical used, one or two clinic visits may be required. The duration of the scan itself is 30 minutes.
Radioisotopes of iodine. They accumulate in the tissues of the thyroid gland during the day. Therefore, in the morning of one day the patient comes to the clinic, takes radiopharmaceuticals orally (drinks), and the next morning a scan is performed.
Radioisotopes of technetium. The substance is administered intravenously and accumulates in the gland within half an hour. After this, scintigraphy is performed.
Important! The use of technetium allows you to undergo an examination and get results in one day. Also, technetium is eliminated from the body much faster than radioactive iodine, and has virtually no side effects such as allergies.
Where is scintigraphy done?
You can undergo thyroid scintigraphy only with a referral from an endocrinologist. This procedure is usually paid for, regardless of the institution in which it is carried out (in a private medical center or a public hospital). Therefore, you should choose a clinic where the examination is performed by qualified specialists using modern high-tech equipment.
Receiving material
It is very important that endocrinologists, surgeons, radiologists and cytologists work together. The purpose of their joint work should be the exchange of information obtained at different stages of examination and treatment for optimal treatment tactics and continuity of observation.
The first stage of the examination is palpation of the neck to exclude formations not related to the thyroid gland. FNA should be performed by an experienced doctor (surgeon or ultrasound specialist). Ultrasound-guided puncture reduces the likelihood of erroneous and, most importantly, false negative conclusions due to the fact that the needle does not enter the pathological focus. Information about the results of ultrasound helps the cytologist to correctly interpret the cellular composition of smears.
Thyroid puncture is performed with the patient lying on his back with a small pillow under the neck and shoulders, the neck muscles are relaxed. This position allows for optimal access to the punctured area. The patient should be warned not to talk or swallow during the procedure. Use 23 gauge needles (with an outer diameter of 0.8 mm). Local anesthesia with lidocaine can be used. Usually, needle pricks in two or three directions are sufficient; in rare cases, multiple “passes” are required to obtain complete material. The results of the study are significantly improved if the punctate is immediately assessed by a cytologist (urgent cytological diagnosis for the presence of cellular material); If defective material is received, a repeat puncture is immediately performed.
To exclude the malignant nature of the lesion, at least two punctures are considered necessary - during the initial examination and over time. The material is spread on the glass in a thin layer. If, during puncture of the thyroid gland, abundant bloody material is obtained (which happens quite often), it is distributed on several glasses, preparing thin preparations, like blood smears. The material containing liquid must be centrifuged and preparations made from the sediment. The quality of smears is significantly improved when using cytocentrifuges such as Cytospin, Cellspin, Rotorfix, etc.
Safety of the procedure
Scintigraphy is a safe procedure, contrary to popular belief. Radioactive substances are eliminated from the body within 24 hours, without causing any harm to healthy tissues and organs. After the examination, it is recommended to drink more fluids to increase urination and speed up the process of removing radiopharmaceuticals. It is also advisable to immediately take a hygienic shower, wash your hair with shampoo, and wash the clothes you wore during the examination.
Scintigraphy is a painless procedure, does not cause much discomfort to the patient and is usually easily tolerated by patients. Testing with technetium is allowed even for small children and infants.
Note: repeated scintigraphy may be required to monitor the effectiveness of the prescribed treatment. Usually the procedure is carried out 2 months after the initial examination.
Competition "bio/mol/text"-2019
This work was published in the “Free Topic” category of the “bio/mol/text” competition 2019.
The general sponsor of the competition and partner of the Skoltech nomination is the Skoltech Center for Life Sciences.
Competition sponsor: the largest supplier of equipment, reagents and consumables for biological research and production.
The audience award was sponsored by BioVitrum.
"Book" sponsor of the competition - "Alpina Non-Fiction"
Undoubtedly, the 21st century is a time of development of scientific and technological progress. As technology improves, so does its widespread availability. Medicine is no exception. Thanks to the development of technologies for diagnosing and treating a wide variety of diseases, we have begun to save those patients who were once among the incurable. However, not all areas of medicine have been so positively affected by progress. Therefore, today we would like to introduce you to such pressing medical issues as overdiagnosis and overtreatment. Now we will focus on only one, but very significant side of this problem - overdiagnosis of thyroid nodules, as well as overtreatment of these nodules and thyroid cancer.
Thyroid scintigraphy results
In conclusion, the radiologist gives a detailed description of the anatomical position, shape and size, structure of the gland and the “hot” and “cold” nodes present in it.
“Hot” nodules accumulate more radiopharmaceuticals, which means they produce more hormones. Such hyperactivity may be a symptom of nodular toxic goiter or toxic adenoma.
“Cold” nodes are clusters of idle cells. The tissue does not absorb radiopharmaceuticals and does not synthesize hormones. Such formations are characteristic of nodular colloid goiter or tumor diseases and require further diagnosis by fine-needle biopsy (tissue sampling for study).
The overall pattern of tissue absorption of the radioisotope allows us to assess the functionality of the thyroid gland as a whole. If the level of saturation is increased evenly, then this is one of the signs of diffuse toxic goiter. A decrease in absorption activity indicates hypothyroidism.
Thyroid pathologies
There are several fairly common pathologies of the thyroid gland. In hypothyroidism, the gland secretes a small amount of thyroxine, the main thyroid hormone. This leads to a slower metabolism and decreased thyroid function. Symptoms of this disease include noticeable weight gain, loss of appetite, constant feeling of cold, depression and fatigue. The person's heart rate also slows down and constipation occurs.
With hyperthyroidism, the opposite phenomenon occurs. The thyroid gland secretes excessive amounts of thyroxine, so metabolism speeds up. Symptoms of the disease include weight loss, rapid heartbeat, and frequent diarrhea.
Thyroid cancer is a malignant tumor that arises from the cells of the thyroid gland. Nuclear tomography can detect dysfunction of this organ.
Most importantly: why is overdiagnosis and overtreatment of thyroid cancer a problem?
Is such excessive detection of thyroid masses a problem? Yes, and very serious. And it got its name - overdiagnosis [19], [20]. And the problem is that the consequence is overtreatment . In fact, it concerns not only the thyroid gland and poses a more serious danger than it might seem at first glance, and as diagnostic methods develop, it becomes more and more widespread, as an endocrinologist says in his article “Just in Case...” V.V. Fadeev [28]. Speaking of thyroid cancer, most patients with papillary thyroid cancer undergo surgical treatment—total thyroidectomy or hemithyroidectomy [21]. However, some studies [22], [23] have shown that when choosing treatment in favor of “active surveillance” in patients with papillary thyroid cancer (which refers to low-risk thyroid cancer) with a diameter of less than one centimeter, the same outcomes of the disease, as well as during surgical operations. In this regard, in 2015, the clinical guidelines of the American Thyroid Association (ATA) first adopted the “active surveillance” strategy for patients with low-risk cancers [24].
Due to the revealed fact that there is quite possibly no need for surgical treatment of such thyroid cancer (and the removal of thyroid cancer is accompanied by serious consequences, which we will discuss later), since 2015, measures have already been taken in the United States to reduce the frequency of overdiagnosis and overtreatment [24 ]. For example, it is already strongly recommended not to screen patients for thyroid cancer who do not have any symptoms, since detection of aggressive types of cancer in this case is extremely unlikely.
Another measure to prevent overtreatment is to change the classification of types of thyroid cancer that behave as benign. In other words, they are no longer called “cancer.” For what? It's all about the patient's psychological reaction. The instinct of self-preservation is the most tenacious instinct of humans and animals. And it is realized largely thanks to fear. Thanks to fear, an antelope runs away from a lion, and a snake bites a potential threat - animals strive to survive. It's the same with a person. By all means, a person wants to prolong his existence on this earth. And the diagnosis of cancer, which society is accustomed to associate with the painful end of life, forces a person to do everything to get rid of this very cancer. In our case, if a person is diagnosed with thyroid cancer, the most persistent thought is to get rid of this torment. And in most cases, the choice falls on complete removal of the thyroid gland, regardless of whether it is necessary. As they say, just in case. And in many cases this is not justified.
One study [25] found that people generally have a general understanding of thyroid cancer, but do not know about its diagnosis and treatment, believing that thyroid cancer is similar in prevalence and mortality to other types of cancer. Fear of further progression of the disease forces the patient to choose radical treatment. Thus, recent studies of non-invasive breast cancer [24], [25], and subsequently papillary thyroid cancer [25], have shown the influence of terminology on the choice of treatment: replacing the term “cancer” in the description of both pathological conditions contributed to the patient’s choice of non-surgical treatment. Thus, this strategy has an impact on the psychological state of patients, thereby preventing overtreatment. Is it possible to live with a cancer diagnosis? How would you answer this question?
Where do so many cases of thyroid cancer come from?
Thyroid cancer ( TC ) is the most common malignant neoplasm of the endocrine system [2]. We increasingly hear that the incidence of thyroid cancer is steadily increasing. And it sounds terrifying, but is it really that simple? You might be shocked at the truth behind these seemingly straightforward scientific facts. And before we understand the true reason for the increase in the incidence of thyroid cancer, it is necessary to become familiar with what types of thyroid cancer exist.
So, let's begin. Now we will need to provide some numerical data, but do not be alarmed by them, everything is extremely simple. In the scientific community, there are five types of thyroid cancer:
- Papillary (80–85% of cases).
- Follicular (10–15% of cases).
- Medullary (5% of cases).
- Poorly differentiated (1% of cases).
- Undifferentiated (0.1–0.2% of cases).
The first two types of thyroid cancer are considered to be the most favorable. And as we can see, they are the most common. They are also called high-grade cancers. Medullary, poorly differentiated and undifferentiated types are considered aggressive forms of thyroid cancer. In our article we will focus only on the first two types of thyroid cancer, since they are the most common.
What does the term “differentiation” mean?
Once upon a time, even before we were born, each of us was a single cell. During intrauterine development, cells increased trillions of times! And each of them acquired its own function: some are responsible for the beating of our heart, others protect our body from external and internal dangers, and still others are responsible for cognitive functions. And there are more than 230 such types of cells! The path that a cell takes from the one that stood at the beginning of our journey to a highly specialized cell that has clear responsibilities is called “ differentiation ”.
As for cancer, if the cells that make up the tumor are highly differentiated, in most cases doctors consider the outcome to be favorable. However, if the tumor consists of poorly differentiated cells, then it is most likely prone to an aggressive course. As already mentioned, the most frequently detected thyroid cancers are highly differentiated.
Papillary thyroid cancer is the most common form: 80–85%. And with the best prognosis. The five-year survival rate of patients with thyroid cancer is 98.1% [2]. What does this mean for the patient? That the most frequently detected cases of thyroid cancer have a favorable outcome!