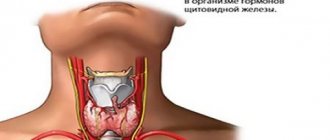
Functions of the gland
The thyroid gland contains iodine and produces iodine-containing hormones necessary for the regulation of metabolism, as well as the growth and development of the body as a whole or its individual tissues. The main functions of the thyroid gland include:
- affects the growth and development of almost all tissues in the body,
- takes part in the functioning of the nervous system and mental activity,
- regulates protein, carbohydrate and fat metabolism in the body,
- affects reproductive function,
- participates in the formation of bone tissue (bone metabolism), is responsible for its strength,
- can lead to mental retardation in the fetus (with iodine deficiency in the mother).
Detailed description of the study
Thyroid nodules (TG) are a widespread pathology. Every year it is diagnosed in approximately 25% of residents of European countries and 20% of residents of the United States. As a rule, most of these formations are benign. These include:
- Hyperplastic colloid goiter - enlargement of the thyroid gland due to the formation of formations consisting of colloidal fluid;
- Thyroid cysts are hollow formations filled with liquid contents;
- Thyroiditis is inflammation of the thyroid tissue;
- Thyroid adenomas are round or oval nodes with a pronounced fibrous capsule.
There are several main reasons for the development of thyroid nodules:
- Iodine deficiency;
- Congenital pathologies of thyroid hormone production;
- Taking medications (amiodarone, lithium) that suppress the synthesis of thyroid hormones.
As a rule, thyroid nodules are asymptomatic. As they grow, patients note an enlargement of the gland itself, in which dense nodes or cysts are detected upon palpation.
There are different forms of thyroid cancer. Thyroid cancer (TC) occurs in less than 10% of cases. There are four main types of thyroid cancer:
- Papillary;
- Follicular;
- Medullary;
- Anaplastic.
Thyroid cancer in most cases also manifests itself as painless nodules. They are often discovered by chance during routine examinations by an endocrinologist or during a preventive ultrasound.
To differentiate malignant and benign thyroid formations, fine-needle aspiration biopsy under ultrasound control is used, followed by cytological examination of the resulting aspirate.
Cytological examination is prescribed in the following cases:
- The presence of a thyroid node or several nodes in patients with normal levels of thyroid hormones;
- Inconsistency between ultrasound examination data and clinical picture;
- Enlargement of the thyroid gland or other changes in the organ.
The material is taken using a special aspiration needle under ultrasound control; control is necessary for targeted extraction of material from the lesion and to eliminate possible errors.
At the National Cancer Institute in Bethesda (USA), a classification system for interpreting the results of FNA of the thyroid gland was developed. The classification included six points assessing the risk of malignancy of nodules.
- DCI - “Uninformative material”, in this case it is necessary to perform a repeat TAB, since the drug has disadvantages in the form of a small amount of material, its poor fixation and other signs that make diagnosis impossible.
- DCII - “Benign formation”, in this case we can talk about a low risk of malignancy. For such patients, clinical and ultrasound monitoring of nodular formations over time and tracking the size of the nodule are recommended.
- DCIII - “Follicular lesion of undetermined significance/atypia of undetermined significance.” The risk of malignancy of the formation is 10 – 30%. Such patients are recommended to undergo repeat FNA, molecular genetic testing or hemithyroidectomy (removal of the thyroid lobe with formation and subsequent pathological examination).
- DCIV - “Follicular neoplasia / suspected follicular neoplasia.” The risk of malignancy of the neoplasm is 25-40%. Such patients are recommended to undergo molecular genetic testing or hemithyroidectomy to clarify the results of the study.
- DCV - “Suspected malignancy”, in this case they speak of a high risk of malignancy (50-75%). This term is used when papillary, medullary, metastatic thyroid cancer or lymphoma is suspected. Upon receipt of such a cytological conclusion, it is recommended to conduct additional laboratory tests, which are prescribed by the attending physician. Surgical treatment (thyroidectomy) is also recommended.
- DCVI - Malignant neoplasm. The risk of malignancy is 97-99%. The presence of undeniable signs of cancer. A thyroidectomy or hemithyroidectomy is necessary.
To form a correct conclusion on the analyzed preparation, it must contain at least six groups of clearly visible cells of the epithelial component.
Cytological examination in the diagnosis of thyroid diseases is highly specific and allows you to accurately differentiate benign and malignant neoplasms, determine the stage of malignancy in order to plan further treatment and management of the patient.
Little "conductor" of a big orchestra
Despite its small size, the thyroid gland plays a large role in the body - the hormones produced in it are involved in almost all processes of the body. The main function of the thyroid gland is to maintain normal metabolism (metabolism) in the cells of the body. Thyroid hormones stimulate metabolism and regulate virtually every process in the body - breathing, eating, sleeping, movement, as well as processes in internal organs - from the heartbeat to the functioning of the reproductive system.
References
- Troshina, E.A., Sviridenko, N.Yu., Vanushko, V.E. and others. Federal clinical guidelines for the diagnosis and treatment of thyrotoxicosis with diffuse goiter (diffuse toxic goiter, Graves-Bazedow disease), nodular/multinodular goiter, 2014. - 25 p.
- Semkina, G.V., Abrosimov, A.Yu., Abdulkhabirova, F.M. and others. Comparative analysis of cytological reports and diagnostic categories of independent cytologists. Clinical and experimental thyroidology, 2013. - No. 3. — P.29-34.
- Singaporewalla, R., Hwee, J., Lang, T. et al. Clinico-pathological Correlation of Thyroid Nodule Ultrasound and Cytology Using the TIRADS and Bethesda Classifications, 2021. - Vol. 41(7). — P.1807-1811.
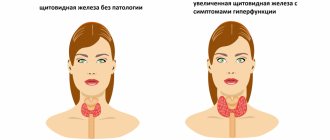
“Floats like a butterfly, stings like a bee”
This motto is fully applicable to diseases of the thyroid gland (the shape of the gland resembles a butterfly). According to world statistics, at least 3% of the population suffers from various diseases of the thyroid gland (increased or decreased function of the gland, nodules). Thyroid diseases, along with diabetes, are the most common endocrine pathology and occur 5-10 times more often in women than in men. The main diseases of the thyroid gland are enlargement (goiter), insufficiency (hypothyroidism) or excess (hyperthyroidism) function, inflammation (thyroiditis) and malignant formations.
“What do you have?”
Is it possible at CELT to puncture the thyroid gland under ultrasound control? Yes, sure. We have very competent specialists in thyroid ultrasound, and we have everything necessary to perform a puncture biopsy of the thyroid gland in any variant.
Can you trust the quality of your cytological reports? We think so. The country's leading specialist in this field, Maria Ilyinichna Bronshtein, works for us as a cytologist. In addition, we are open to control and are not afraid (unlike some other clinics) to give patients glass preparations with smears, which they can consult in any clinic in our country and abroad.
"Gordian knot" of the thyroid gland. Does it need to be “cut”?
Does every nodular goiter need to be operated on? No, not everyone. With the introduction of ultrasound into clinical practice, nodules began to be found in the thyroid glands of a very large number of patients. The percentage of diagnosis of nodular forms of goiter has increased sharply, but the approach to their treatment has remained the same. Previously, about 15-20 years ago, nodules in the thyroid gland were found, as a rule, when they reached a large size and became visible to the naked eye or could be easily palpated. This is possible when the size of the node exceeds 3-4 cm in diameter. Of course, such nodes need to be removed promptly. But what to do with small nodules measuring 0.7–1.5 cm, which do not affect the patient’s health in any way, needs to be understood on a case-by-case basis. They definitely need to do a high-quality ultrasound of the thyroid gland. If a nodule in the thyroid gland inspires any suspicion in a specialist, it must be punctured. Further treatment tactics depend on the results of the puncture.
What are the indications for surgical treatment for diffuse toxic goiter and autoimmune thyroiditis? In case of diffuse toxic goiter, indications for its surgical treatment are the ineffectiveness of conservative treatment for 6-9 months, intolerance to medications used for this treatment, large size of the goiter, and the patient’s pregnancy. In case of autoimmune thyroiditis, there are very few indications for surgery: a large goiter with compression of the neck organs, the presence of nodes suspicious for cancer against the background of autoimmune thyroiditis.
Can you operate on thyroid cancer? Can. This operation can be performed both by me and by CELT oncologist Igor Vladimirovich Soldatov.
Preparation for the procedure
No preparation is required for thyroid scintigraphy, which uses the technetium isotope 99Tcm.
If the study uses iodine isotopes, then:
- A month before the proposed test, you stop taking thyroid hormones and medications that contain iodine. This point must be discussed with the attending physician.
- If you are taking Cordarone or other antiarrhythmic drugs based on amiodarone, in agreement with your doctor, they are excluded from your prescription list at least 3 months before the examination.
- A week before scintigraphy, the use of sulfonamides, aspirin, Mercazolil, and drugs containing a nitrate component (nitrosorbitol, nitroglycerin, Cardiquet, etc.) is undesirable.
Indications and contraindications
It is important for the endocrinologist to know what an MRI will show if, during the initial examination, he discovered a significant enlargement of the organ. The doctor may also refer you for examination if there are sharp fluctuations in weight (both during weight loss and weight gain), tachycardia, or heartbeat disturbances; with rapid changes in mood, irritability, fatigue. An MRI examination will be required before surgery - the doctor must know exactly the location, as well as the degree of enlargement and compression of the organs.
As for contraindications, there are several of them. It is prohibited to do tomography:
- pregnant women;
- patients whose body contains a device or device made of metal - a pacemaker, insulin pump, pins, wires, implant;
- people suffering from mental disorders.
For those who experience claustrophobia, thyroid testing is performed using an open-circuit machine. They resort to such an examination if the weight or dimensions of the patient do not allow him to be placed inside the device.
“Measure a hundred times - cut once”
How does your thyroid surgery technique differ from others? This is a very difficult question and cannot be answered in a few words. In general, we proceed from the provisions of the school of endocrine surgery, which considers each endocrine organ as vital for the whole organism and strives to preserve the function of this organ as much as possible. Therefore, we never deprive a patient of functionally suitable internal secretion organs unless absolutely necessary; we try to operate sparingly, with minimal trauma for the patient and predicting the fullness of his life after the operation. Further, during operations on the thyroid gland there can be a number of complications that are extremely unpleasant for the patient, leading to his disability. Therefore, approaching these operations as relatively simple and easy to perform is unacceptable. These operations should be performed only by a highly qualified endocrinologist surgeon who knows the degree of risk of complications and is proficient in the technique of these surgical interventions. In addition, in some cases, during the operation, the surgeon has to adjust to a different volume, dictated by oncological indications. Thus, a surgeon operating on the thyroid gland must be fluent in both a minimally invasive technique that is justified for the further function of the gland and does not lead to complications, as well as the full range of advanced oncological interventions. This is in the best interests of the patient.
Are the scars noticeable after your surgeries? No. We try to make minimal incisions and use plastic surgery techniques. In the vast majority of our patients, the scars are invisible.
Is it possible to perform thyroid surgery endoscopically? Can. But today, all over the world, these operations are in the experimental stage. Endoscopic removal of parathyroid adenomas has become more widespread.
Are thyroid surgeries always performed under general anesthesia? This is decided individually and depends on the size of the goiter, concomitant pathology and the experience of the surgeon. We use anesthesia, local anesthesia and combined anesthesia.