Introduction
Recently, the understanding of the impact of COVID-19 on other organs has expanded significantly, as a number of studies have demonstrated that more than half of patients with COVID-19 have various liver lesions [6]. A new study has shown that the SARS-CoV-2 virus can bind to angiotensin-converting enzyme 2 (ACE2) on cholangiocytes, leading to their dysfunction and causing a systemic inflammatory response causing liver damage [7]. As of March 10, 2021, seven relatively large studies have reported the clinical characteristics of patients with COVID-19 who experienced liver injury [8–14]. These studies reported elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels ranging from 14% to 53% [8,9,11,14]. Pathological evaluation of liver biopsies from patients who died from COVID-19 revealed moderate microvesicular steatosis and mild lobular and portal inflammation, indicating that SARS-CoV-2 infection could be a possible cause of these changes [15]. However, until now, data on the clinical and laboratory characteristics of liver failure in patients with COVID-19 are extremely scarce. Therefore, the aim of this study was to elucidate the clinical course and liver function test parameters of COVID-19 patients admitted to a single referral hospital in Shenzhen, China.
Study design and patient selection criteria
A cross-sectional study was conducted at the Third People's Hospital of Shenzhen from January 11, 2021 to February 21, 2021, which included 417 patients diagnosed with COVID-19 in accordance with WHO temporary recommendations [16]. Patients with more than one abnormal liver function test result from admission to the end of February 2021 were included in the study. The study was approved by the ethics committee of the Third People's Hospital of Shenzhen (2020 019).
Analysis that shows that the liver is not coping
To find out whether your liver can cope with the daily load of food, drinks and medications or not, you need to take a biochemical blood test for the liver enzymes ALT and AST. Ultrasound is not informative in this regard, because it does not reflect the inflammatory process.
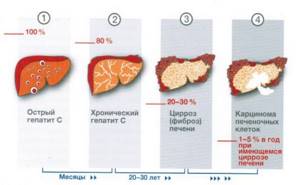
In a healthy body, ALT and AST are located inside hepatocytes (liver cells), as in capsules. If the analysis shows an increase in both indicators, then the liver cells are destroyed and the enzymes “leak” into the blood. This, for example, happens with hepatitis - viral, alcoholic, drug - and with cirrhosis of the liver.
AST, in addition to the liver, is found in the heart, kidneys, pancreas, brain, and muscles. If this enzyme is elevated and ALT is normal, the problem may not be in the liver at all. It is necessary to exclude problems of other organs.
Low levels of ALT and AST in the blood serum occur during pregnancy, fasting and vitamin B6 deficiency.
If the readings are higher than normal, you need to contact a gastroenterologist and look for the cause. If the enzymes are within normal limits, your liver is fine and no further testing is needed.
Liver test parameters and abnormalities
Abnormalities in liver function tests were defined as increased serum levels of the following parameters: ALT > 40 U/L, AST > 40 U/L, gamma-glutamyl transferase (GGT) > 49 U/L, alkaline phosphatase (ALP) > 135 U/L d and total bilirubin (TB) > 17.1 µmol/l. Since COVID-19 is a new emerging infectious disease, no consensus and guidelines have yet been developed for the classification of liver injuries. This study examined 3 types of liver disorders: hepatocellular, cholestatic and mixed. Hepatocellular type was diagnosed when ALT and/or AST levels exceeded three times the upper limit of normal (ULN); cholestatic – with levels of alkaline phosphatase or GGT exceeding twice the ULN; mixed - in cases where both conditions described above were combined (anomaly (1) type). To further describe the characteristics of liver function tests, increases in ALT, AST (>3 ULN), ALP, GGTP, OB (>2 ULN) were defined as liver injury. Because elevations in liver enzyme levels in patients generally ranged from mild to moderate, additional parameters were introduced. In the hepatocellular type of disorders, AST/ALT activity relative to ULN was higher than ALP/GGT activity; in cholestatic it is the opposite (type 2 anomaly). Because the presence of underlying liver disease could influence the results, patients with chronic hepatitis B and alcoholic/non-alcoholic fatty liver disease (NAFLD) were excluded from the study. NAFLD was identified using ultrasound or computed tomography assessment of steatosis after excluding both secondary causes and daily alcohol consumption ≥ 30 g in men and ≥ 20 g in women [20]. Hepatitis B virus infection was determined by the presence of viral surface antigen [21]. In studying the effects of drugs on liver injury, inverse probability weighting (IPW) was used to account for potential confounding factors and eliminate selection bias based on disease severity at admission. All statistical analyzes were performed using STATA/SE software version 16.0 (StataCorp. 2021. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). Two-sided α values less than 0.05 were considered statistically significant.
AST enzyme assay
Biochemical analysis helps determine the presence of AST in human blood.
Blood for this enzyme is taken from a vein, in the morning and on an empty stomach. Blood is collected using a standard method. Directly during a blood test, plasma is separated from the rest of the formed elements, after which the amount of AST in the blood is determined using chemical elements.
Biochemistry usually gives results the next day. A qualified doctor will easily decipher the test readings.
How to properly prepare for the analysis?
- Stop eating 8 hours before the test, that is, the night before. Since the study takes place in the morning and on an empty stomach,
- 24 hours in advance, give up alcohol, fatty and fried foods,
- Stop physical activity and remain emotionally calm,
- Before analysis, you can drink only clean drinking water without gas,
- It is recommended to stop taking any medications 10-14 days in advance. If this option is not possible, then be sure to notify your doctor.
- In addition, you need to inform your doctor about allergies to any medications and about your pregnancy status.
It is unacceptable to take an analysis within 2-3 hours after certain procedures:
- Ultrasound,
- Rectal examinations,
- Physiotherapy,
- Fluorography,
- Radiography.
What can affect the result?
- Physical activity on the eve of the test,
- Use of certain medications
- The use of drugs such as echinacea and valerian,
- Increased amounts of vitamin A,
- Recent heart surgery.
Purpose of analysis
Aspartate aminotransferase analysis is prescribed to detect and determine the extent of certain diseases, including:
- Liver damage analysis,
- Detection of liver cell death (cirrhosis),
- Detection of hepatitis,
- In order to find out the causes of jaundice (damage to liver tissue or the functioning of the circulatory system),
- Monitoring the effectiveness of therapy,
- Determining the effects of certain medications on the liver,
- Diagnosis of diseases of the cardiovascular system.
The study of AST using biochemical analysis allows us to detect the destruction of cells (cytolysis) of the heart, as well as liver tissue. An increase in the AST index upon impact on other organs is not detected.
Important! The main task of the analysis is to detect tissue destruction, diagnose and identify diseases.
Clinical characteristics of patients with COVID-19 on admission
On admission, approximately half of the patients had abnormal liver function tests, and 21 (5%) had liver injury. Patients with abnormal test results were most often men over 40 years of age (p < 0.05) with a higher body mass index. These patients also tended to have underlying liver disease, including NAFLD, alcoholic liver disease and chronic hepatitis B (p = 0.001), and many presented with cough (p = 0.04). Liver test results on admission were within 1–2 × ULN in most patients, with only a few (<4%) exceeding 2 × ULN. Elevated GGT levels on admission were more significant: 53 (12.71%) had 1-2 × ULN, 5 (1.2%) had 2-3 × ULN and 10 (2.4%) had more than 3 × ULN .
For what indications is the test prescribed?
Observing certain diseases in a patient, the doctor can send him for a biochemical analysis of AST:
- Kidney failure
- Injuries to the chest and abdominal cavity,
- All liver damage
- Diseases of the cardiovascular system,
- Infections,
- Malignant tumors
- In preparation for surgery,
- Skin allergies,
- Jaundice,
- Chronic pancreatitis,
- Long-term treatment with chemicals and antibiotics,
- and other factors.
Clinical features of patients with COVID-19 and results of liver tests during hospitalization
Among 318 COVID-19 patients with abnormal liver function tests, 26.7% developed severe pneumonia during hospitalization. 20.75% of abnormalities were hepatocellular, 29.25% were cholestatic, and 43.4% were mixed types. During hospitalization, deviations from the norm became more pronounced in the levels of ALT, AST, OB and GGT: a threefold excess of the ULN of these indicators was observed in 33 (10.38%), 18 (5.66%), 9 (2.83%) and 37 (11.64%) patients, respectively.
Reasons for the downgrade
A drop in the levels of these enzymes is quite rare. But with certain diseases, AST may decrease below 15 U/l.
A decrease indicates the following diseases:
- Advanced form of liver cirrhosis,
- Death of liver tissue (necrosis),
- Lack of vitamin B6,
- Decrease in the number of working hepatocytes,
When will additional tests be needed? In certain cases, the doctor will not be able to make a diagnosis without sending you for additional examinations.
In case of doubtful tests, they are sent to:
- Determination of ALT, the same important blood enzyme, but mostly located in the heart. If ALT is increased more than AST, then destruction of liver tissue is likely, and in the case of lower corresponding indicators, a heart attack is possible.
- MB reaction of creatine phosphokinase (an enzyme very important for the skeleton and heart muscles). Observe its dynamics.
- Complete ultrasound of the liver, kidneys and heart,
- Testing for troponins . Post-infarction enzymes. Even if their increase in some hours after a heart attack is not great, this still indicates the possible death of the heart muscles,
- Pigment and fat analysis , as well as carbohydrate analysis, are carried out.
How to reduce
It is very important that an AST level higher than normal in the blood does not mean that this is a separate disease, but always follows the progress of some disease. So there are no comprehensive actions aimed specifically at reducing AST.
A high level of AST signals that the cells of the heart, liver or muscles are destroyed. Only restoration of damaged tissues can bring the AST condition back to normal. A qualified doctor can determine the damaged organ based on AST readings.
If the AST level is too high, then this is not the cause - but only a consequence of some pathology.
Clinical characteristics of patients with COVID-19 and liver injury during hospitalization
Among 90 patients with COVID-19 and liver damage during hospitalization, approximately half had severe disease. Elevations of ALT and GGT were detected frequently (more than 3 × ULN in 37% and 41% of patients, respectively), while increases in AST and OB were somewhat less common (more than 3 × ULN in 20% and 10% of patients, respectively). The increase in ALP levels was not indicative, since the level of this enzyme exceeded three times the ULN in only 1 patient. Use of antibiotics, NSAIDs, Chinese herbal medicine, and interferon were associated with progression to severe disease (p <0.001 to 0.04). Moreover, in 10 (23.26%) cases of severe disease, multiple organ failure was observed, of which three patients died (one had liver failure). In addition to respiratory failure, these 10 patients developed other complications: liver failure (2/10), septic shock (9/10), heart failure (4/10), renal failure (8/10), gastrointestinal bleeding (1 / 10) and disseminated intravascular coagulation syndrome (2/10). With the exception of respiratory failure, most of these complications, including liver failure, were associated with severe secondary infections in the intensive care unit.
AST norm indicator
The normal level of AST varies depending on the gender and age category of a person. Factors that increase the concentration of AST, in the vast majority of cases, are diseases and pathological processes.
The concentration levels of this enzyme in the human body are given below (Table 1):
Table 1 Normal AST values
| Category of people | Children under 9 years old | Conjured up | Men | Women |
| Normal values Units/l | less than 55 | Up to 140 | 15-31 | 20-40 |