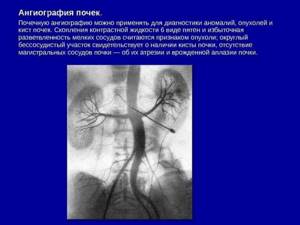
Brief description of the procedure
Total procedure time: 30 min Use of contrast agent: yes, intravenously Preparation and preliminary examinations: no

CT angiography of the renal arteries with bolus contrast and 3D reconstruction is a highly informative way to assess the condition of the vessels in the kidneys. Multispiral scanning, unlike conventional angiography, takes only about 2 minutes, involves less radiation exposure and is more accurate. The scanner takes many pictures, which, after processing in the program, are converted into multi-plane images or three-dimensional visualization. Since the pictures are taken at the time of contrast, the doctor sees the smallest deviations from the norm. CT angiography of renal vessels helps to make an accurate diagnosis, perform preoperative planning, and evaluate treatment results.
Angiography of renal vessels and renal arteries

A method such as angiography of the renal vessels and renal arteries is used in cases where other diagnostic techniques (X-ray, ultrasound, MRI, etc.) do not produce results. Angiography can reliably detect the presence of tumors, injuries, and developmental anomalies. It can be prescribed to both adults and children.
This diagnosis is a study of blood vessels using a contrast agent and radiography. The contrast entering the circulatory system of the kidneys improves the visualization of blood vessels on X-rays. This allows you to evaluate the anatomy and functioning of the organ under study, as well as the structure and functioning of its vessels.
Angiography is an invasive procedure performed under anesthesia. After the procedure, the patient may experience some adverse reactions. You need to take them calmly, as they are the norm and go away on their own 2-4 hours after the procedure. Such reactions include: headaches, iron taste in the mouth, weakness, dizziness, mild fever. However, the patient is under medical supervision for 5-6 hours after the procedure in order to stop more serious complications in a timely manner.
Why is renal artery angiography required?
The study is carried out to determine the condition of the renal arteries, i.e. main arteries that supply blood to the kidneys.
Angiography of the renal arteries may show the presence of:
- aneurysm (expansion of a vein or artery by more than 50% of the proper diameter);
- abnormal connections between an artery and a vein (fistula or fistula);
- thrombi (blood clots) in the lumen of the arteries;
- narrowing of the blood vessels in the kidneys (renal stenosis);
- benign or malignant tumors;
- active bleeding from the kidney.
Renal angiography is also used to study donors and patients before kidney transplant surgery, to determine the number of arteries and veins in each kidney.
When is renal angiography prescribed?
Angiography may be prescribed for the following purposes:
- studying the renal vascular system before the upcoming operation;
- identifying the cause of renovascular hypertension;
- assessment of the renal vascular system in chronic diseases of this organ or renal failure;
- identifying tumor-like neoplasms and clarifying their type (tumors or cysts);
- control over the condition of transplanted kidneys (kidneys).
Direct indications for angiography are:
- blood in the urine for an unknown reason;
- suspected kidney cancer;
- hydronephrosis;
- anomalies of kidney development identified by ultrasound
, MRI; - kidney tuberculosis;
- arterial hypertension.
RENAL ANGIOGRAPHY
RENAL ANGIOGRAPHY
(Greek, angeion vessel + grapho write, depict; syn.
renovasography
) - radiography of the kidney and its blood vessels after the introduction of a contrast agent into them. P. a. used to assess the condition of the kidneys and their arterial and venous vessels in cases where conventional methods rentgenol, research do not allow us to establish the nature and localization of patol, the process or when the possibilities and scope of surgical intervention remain unclear.
The first rentgenol, study of the vessels of a macroscopic specimen of a pathologically altered kidney was carried out in 1913 by E. Hauch. In 1923, Berberich and Hirsch (J. Berberich, S. Hirsch) published the results of the first successful intravital P. a. However, only in 1929, after the development of the method of translumbar aortography (see) by R. Dos Santos, Lamas and Caldas (AS Lamas, J. R. Caldas), the study of the kidneys using angiography became widespread in wedges, practice. P. a. is especially widespread. began to be used in 1953, when S. Seldinger proposed the method of percutaneous puncture catheterization of the aorta through the femoral artery (see Seldinger method). The first successful P. a. in the USSR was performed in 1956 by N.A. Lopatkin.
Renal angiography has acquired leading importance in the recognition and differential diagnosis of various diseases of the kidneys and perinephric tissue (perinephric fat body, T.; corpus adiposum pararenale): malignant and benign tumors, cysts, hydronephrosis, chronic inflammatory diseases, malformations, injuries and lesions of the renal vessels of various etiologies.
P. a. Contraindicated if the patient is hypersensitive to iodine-containing contrast agents. Carrying out P. a is not justified. in severe condition of the patient and in generalization of the patol process. It is not recommended to carry out P. a. with severe atherosclerosis.
Two main methods of contrasting the bloodstream of the kidney have been developed: semi-selective P. a. and selective P. a. Vessel catheterization in both cases is carried out using the Seldinger method (by percutaneous puncture of the femoral artery, the catheter is inserted into the abdominal aorta or into the renal artery). The choice of method for introducing a contrast agent into the bloodstream of the kidney is determined by the specific task of the study and the nature of the blood supply to the kidney.
Rice. 1. Semi-selective renal angiograms for adenocarcinoma of the left kidney: a - arterial phase, semi-selective filling of the main (1) and left accessory (2) renal arteries with a contrast agent, characteristic dilatation of the vessels of the left kidney is noted; b — parenchymal phase, the tumor of the left kidney (indicated by arrows) and unaffected renal parenchyma are contrasted. Rice. 2. Semi-selective renal angiograms for chronic right-sided perinephric abscess (fragment): a - arterial phase: semi-selective filling of the main (1) and accessory (2) arteries of the right kidney with a contrast agent; avascular zone in the upper outer part of the kidney (3); b — parenchymal phase: displacement of the renal cortex inward by an abscess; the vessels of the abscess capsule are visible (indicated by the arrow).
With semi-selective PA, or floor-by-floor aortography, 30-40 ml of a 76% contrast agent solution is injected into the aorta at the level of the origin of the renal arteries at a rate of 20-25 ml/sec through a catheter with 4-6 side holes and an obstructed end or through a catheter with a loop at the end. Under these conditions, relatively isolated simultaneous contrasting of the main and accessory renal arteries on both sides is achieved (Fig. 1, 2). With this method P. a. It is not always possible to obtain a complete understanding of the nature of intraorgan vascular disorders and it is impossible to conduct rentgenol, a study in two projections due to the superimposition of images of both kidneys on each other.
Rice. 3. Selective angiogram for adenoma of the left kidney (direct projection): late arterial phase with a well-contrasted vascular system of the kidney; in the middle outer part of the kidney, the vascular pattern is depleted due to the expansion and compression of the arteries by a rounded avascular formation (indicated by the arrow). Rice. 4. Selective renal angiograms for polycystic left kidney (direct projection): a - arterial phase: the entire arterial bed of the kidney is well contrasted, including deformed, separated vessels; b — parenchymal phase: against the background of well-contrasted renal parenchyma, multiple round low-contrast zones are revealed - cysts (indicated by arrows).
Selective P. a. (selective arteriography of the kidneys) is based on selective catheterization of the renal artery followed by the injection of 10-15 ml of a 60-76% contrast agent solution into it at a rate of 5-8 ml/sec. For selective P. a. use thin catheters with a standard beak-shaped bend of the apex with end and side openings. The advantage of selective P. a. It is possible, with a small amount of contrast agent, to obtain an isolated image of the kidney with many details of the structure of the vessels in two projections (Fig. 3, 4). The disadvantage of the method is the impossibility of obtaining simultaneous images of the bloodstream of both kidneys. In addition, the method does not allow us to determine patol, a process localized in the perinephric tissue, and the connection of patol, a process in the kidney with adjacent organs and great vessels. Frequent development of the renal artery also limits the use of this method.
For the differential diagnosis of benign and malignant kidney tumors, the method of selective renal pharmacoangiography is used, during which 0.1 ml of 0.001% adrenaline solution is first injected into the renal artery through a catheter, which causes a short-term spasm of only unaffected kidney vessels. With the subsequent introduction (after 10-20 seconds) of a contrast agent, the tumor vessels are better contrasted against the background of spasmodic normal vessels.
Regardless of the method of administration of the contrast agent for P. a. water-soluble, tri-iodinated contrast agents are used: triombrine (urografin, isotrast, urotrast), etc. The total amount of contrast agent depends on the patient’s body weight. The day before the P. a. determine the patient's sensitivity to the contrast agent. Immediately before the examination, premedication is carried out, then a survey X-ray of the lumbar region is performed with the patient in the supine position, which makes it possible to clarify the exposure and check the correct position of the patient. Catheterization of vessels and marking of the area under study is carried out under the control of X-ray television (see Television in medicine). After ensuring the correct position of the catheter, contrasting of the vessels and serial radiography are performed.
The main requirement for P. a. — obtaining a separate and clear x-ray image of the kidneys in all three phases of angiography. In the arterial phase, an image of the renal arteries is obtained; in the next, parenchymal (capillary) phase, the contrast agent fills the interlobular arteries, afferent and efferent glomerular arterioles, capillaries and venules of the kidney, which provides an intense contrast image of its parenchyma. In the last venous phase, the contrast agent enters the venous bed, and an image of the kidney veins appears on the x-ray. If it is necessary to obtain a clearer image of the renal venous system, they resort to catheterization of the renal vein (see Cavography). Obtain an x-ray image of all phases of P. a. allows the use of seriographs and X-ray machines that provide shooting speeds of up to 3 images per 1 second, with a shutter speed of about hundredths of a second. Shooting speed at P. a. in the first 2 sec. is 2-3 shots in 1 second, in the next 6-7 seconds. — at least 1 photo per 1 second. Duration of shooting of all phases of P. a. is 8-9 seconds.
Complications with P. a. due to ch. arr. errors during vascular catheterization (local hematoma, prolonged spasm of peripheral arteries, thrombosis of the great vessels); cases of toxic effects of the contrast agent are extremely rare.
See also Kidneys, research methods.
Bibliography:
Akkerman G. L. and Romankin V. P. Aneurysms of the renal arteries, Vestn, rentgenol, i radiol., No. 4, p. 45, 1976, bibliogr.; Kuchinsky G. A., Matveev B. P. and Dolgushin B. I. Diagnostic capabilities of arteriography for metastatic lesions of the kidney, ibid., No. 2, p. 66, 1977, bibliogr.; Panikratov K.D. et al. Angiographic study in hydronephrosis, ibid., No. 4, p. 35.1976; Perelman V.M., Portnoy L.M. and Rozenshtraukh L.S. Current state of X-ray diagnostics in urology, ibid., p. 8; Guide to angiography, ed. I. X. Rabkina, p. 223, M., 1977; Abrams HL Renal tumor versus renal cyst, Cardiovasc. Radiol., v. 1, p. 59, 125, 1978; Ekelund L. a. Jons son K. How is renal carcinoma detected? Int. Urol. Nephrol., v. 9, p. 3, 1977; Handbuch der medizinische Radiologie, hrsg. v. L. Diethelm, Bd 13, T. 1, B., 1973; Lehrbuch der Rontgendiagnostik, hrsg. v. HR Schinz ua, Bd 5, S. 523, Stuttgart, 1965; Olsson O. Multiple expanding renal lesions, Acta radiol. (Stockh.), v. 17, p. 481, 1976; Radiology and the kidney, some present concepts, ed. by C. J. Hodson, v. 5, Basel - NY, 1977; Seldinger SI Catheter replacement of the needle in percutaneous arteriography, Acta radiol. (Stockh.), v. 5, p. 368, 1953.
G. A. Kuchinsky.
Preparation for the procedure
Unlike simple radiography, which does not require special preparation, you need to start preparing for kidney angiography 2 weeks in advance, namely, completely eliminate alcoholic beverages from your diet. There are other features of preparation.
- A week before the procedure, you need to stop taking medications (if any were prescribed for treatment) that thin the blood.
- Five days before the procedure, you need to undergo the following examinations: echocardiography
,
ECG
,
fluorography,
blood test for coagulation, general,
biochemical
, Rh determination, for the presence of infections (hepatitis, HIV, syphilis). - Two days before the procedure, you need to undergo a test to detect an allergy to the contrast agent (for this, the patient will be given a small dose of contrast).
- Angiography involves puncturing the skin. The doctor will indicate in which area it will be performed. The patient will have to remove hair from this area of skin the day before the procedure.
- The night before the procedure, you should take a sedative and an antihistamine.
- On the morning of the procedure, the patient is given a cleansing enema.
- Immediately before angiography, you need to empty your bladder.
- On the day of the procedure, you should not eat or drink anything in the morning.
CT scan of the renal arteries with contrast
Vascular angiography is performed using an iodine-containing dye. The contrast is injected into the vein as a bolus using an automatic syringe. Before a CT scan of the renal arteries, the patient must donate blood for a creatinine level test. If the levels are elevated, examination is prohibited, as there is a risk of problems with removing the drug from the body.
Other contraindications to renal angiography:
- pregnancy at any stage;
- iodine intolerance;
- severe form of renal or liver failure;
- pronounced thyrotoxicosis.
In order for a CT scan of the renal arteries with contrast to take place without negative health consequences, you need to properly prepare for it. If the patient suffers from diabetes and takes metformin, it is necessary for the endocrinologist to cancel or replace this drug with another two days before the angiography of the renal arteries.
4 hours before the examination you must abstain from food and liquid. Shortly before leaving home, you can have a light snack. Immediately before the procedure, you must empty your bladder.
Angiography of the renal vessels can affect the composition of breast milk, so nursing mothers are advised to take care of the baby’s nutrition in advance, and after a CT scan of the renal arteries, they will have to skip the next two feedings while expressing milk.
Methods of conducting research
There are several techniques for doing renal angiography.
Transfemoral aortography
For this diagnosis, a contrast agent is injected into the femoral artery. For research it is necessary that:
- the patient lay on his back;
- The administered anesthesia took effect.
Next, the skin is punctured, a catheter is inserted and contrast is supplied to the vessels. In the first minutes of its spread, an arteriogram and a nephrogram are performed. At the end of the procedure, a venogram is performed. Five minutes after the first radiograph, an excretory urogram is performed.
Translumbar aortography
This method differs from the previous one in that the puncture is performed in the lumbar region.
The patient lies on his stomach, extends his left arm along the body, and his right arm to the side (to record pressure and pulse). After the onset of anesthesia, a puncture is performed and a contrast agent is injected. Next, images are taken in the same way as with transfemoral aortography.
Indications
Ultrasound of the renal arteries is prescribed by doctors:
- to examine for the presence of vascular damage from impacts;
- when the patient complains of discomfort in the lumbar region or severe pain in the kidney area;
- for preventive diagnostics for people with heart diseases;
- if a renal infarction is suspected.
| Service | price, rub. | Promotion Price |
| “Healthy Legs” program (duplex scanning of the veins of the lower extremities with assessment of valves and perforating veins and duplex scanning of the arteries of the lower extremities) | 3200 rub. | 3000 rub. |
| Ultrasound triplex scanning of N/C veins with assessment of valves and perforating veins | 2500 rub. | |
| Ultrasound triplex scanning of veins of the upper extremities | 2000 rub. | |
| Ultrasound triplex scanning of the arteries of the lower extremities with measurement of the brachiomalleolar index (BMI) | 2000 rub. | |
| Ultrasound triplex scanning of the arteries of the upper extremities | 2000 rub. | |
| Ultrasound duplex scanning of the arteries of the aorto-iliac segment | 1900 rub. | |
| Ultrasound duplex scanning of the abdominal aorta and visceral arteries | 1900 rub. | |
| Ultrasound duplex scanning of the inferior vena cava | 1700 rub. | |
| Ultrasound duplex scanning of the iliac vein | 1700 rub. | |
| Ultrasound duplex scanning of the renal arteries | 1700 rub. | |
| Intracranial duplex of cerebral vessels | 2500 rub. | |
| Ultrasound of neck veins | 2500 rub. | |
| Ultrasound of the brachiocerebral arteries (BCA) | 2500 rub. | |
| Heart ultrasound or echocardiography for adults | 2400 rub. | |
| Comprehensive neck diagnostics (MRI of the cervical spine, MRI of neck vessels, ultrasound examination of neck vessels, ultrasound of the thyroid gland and soft tissues of the neck, consultation with a neurologist) | 13200 rub. | 9500 rub. |
Contraindications for carrying out
Dynamic indirect angiography of the kidneys is a rather complex procedure that cannot be prescribed if the following contraindications are present:
- pregnancy (all trimesters);
- pulmonary tuberculosis;
- poor blood clotting;
- vascular atherosclerosis;
- renal, pulmonary, liver failure;
- allergy to iodine;
- serious condition of the patient (caused, in particular, by cancer);
- arrhythmia, angina pectoris and other pathologies of the cardiovascular system in severe form.
How is an ultrasound of the renal vessels performed?
Ultrasound of the renal vessels is performed while sitting, sometimes lying on the side. The diagnostician applies a gel to the area of examination for smoother gliding and unhindered passage of the ultrasound signal to the patient’s organs. Next, the diagnostician, moving the sensor in different directions and at different angles, receives all the necessary data. This is a painless method, during which the patient does not worry about anything. The study lasts about 20-30 minutes. After the scan, the patient returns to his normal lifestyle.
Decoding the results
When interpreting the results of angiography images, it is important to consider the following:
- How clearly are the vessels visible, their contours, is there any interruption in the image.
- Are there any shadows? If so, what size are they, where are they located, how dense are they?
- The nature of the distribution of the contrast agent: whether it enters the capillary system or immediately rushes into the vein, whether it enters the soft tissues or remains in the vascular system.
A correct conclusion based on angiography can only be made if the contrast agent was injected evenly and distributed throughout all vessels, the aorta and renal arteries.
An isolated examination of certain vessels and canals is carried out only if the condition of the other kidney is reliably known based on a set of other studies. Most often, in order to most accurately interpret the images, several specialists work on them: a radiologist, a vascular surgeon, a nephrologist.
Diagnostic results
After conducting MSCT of the renal arteries and adrenal glands with contrast, the radiologist makes a detailed interpretation of the obtained images with a description of all vascular structures and areas of examination. After some time, when ready, the result of the study is given to the patient, his relatives or the attending physician in the form of printed images and a written report. The result of such a computer scan is an important document for the attending physician, necessary in order to decide on a further strategy for diagnostic and treatment measures.
results
The result of the ultrasound of the renal vessels will be a written conclusion from the doctor. In it, the doctor will note all identified pathologies and deviations from the norm. The patient will receive the results of the Doppler examination immediately upon completion of the diagnosis. If he has questions, the ultrasound doctor will always be able to comment on the pathologies found and tell him which specialist should be contacted for a final diagnosis.
Author: Telegina Natalya Dmitrievna
Therapist with 25 years of experience









