Doppler examination is another version of ultrasound, which is based on the Doppler effect (the ultrasound signal is reflected from elements of moving blood). This method is non-invasive, completely safe, absolutely painless and does not require special preparation from the patient.
Using a Doppler study, you can evaluate:
- Size, diameter and thickness of the walls of blood vessels and possible disturbances in their structure
- Blood flow speed
- Increased or decreased vascular tone
Doppler examination is often prescribed for pregnant women who have multiple pregnancy, late toxicosis, gestosis, fetal developmental delay, oligohydramnios, fetal size that does not correspond to the norm for the duration of pregnancy, or premature maturation of the placenta.
Doppler examination is also prescribed for patients with chronic diseases, such as, for example, diabetes. In addition, Doppler testing can predict and help prevent a baby's heart defects or other developmental abnormalities of the child's cardiovascular system.
CLINICAL STANDARDS COMMITTEE

The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) is a scientific organization that promotes clinical practice in ultrasound, training and research in diagnostic imaging in women's health.
The ISUOG Clinical Standards Committee (CSC) was created to develop Practice Guidelines and Consensus Statements as educational recommendations that provide healthcare professionals with a common approach to diagnostic imaging.
They are intended to reflect provisions reviewed by ISUOG and considered best practice at the time of publication. Although every effort has been made by ISUOG to ensure the accuracy of the text of the manual in its publication, however, neither the Society itself nor any of its employees or members accepts legal liability for the consequences of any inaccurate or misleading information, options or statements published by the CSC.
ISUOG guidelines do not purport to set legal standards in health care because the interpretation of the evidence contained in the guidelines may be influenced by individual circumstances and the availability of resources. Approved manuals may be freely distributed with permission from ISUOG ( [email protected] ).
Doppler ultrasound modes: D-mode, color mapping, B-flow, etc.
Topic: ultrasound examination of organs and tissues (instructions for use).
Doppler mode
makes it possible to determine the speed and direction of blood movement. Measuring blood flow velocity without error is possible if the angle between the direction of the ultrasound beam and the direction of blood flow is 0. The more this angle approaches 90°, the greater the error will be.
Spectral Doppler echography
(spectral Doppler, D-mode) allows you to assess blood flow velocities in the vessels and represents a curve of changes in the Doppler frequency shift unfolded over time. It is accepted that the blood flow directed to the sensor is displayed on the monitor screen above the zero line and, accordingly, from the sensor - below this line. There are pulsed and constant wave Dopplerography.
Pulse-wave Doppler
(Pulsed Wave Doppler, PW) makes it possible to observe blood flow in a certain area of the vessel and at a certain speed.
The disadvantage of this method is the limitation of the recorded speed and significant difficulties in finding vessels, especially in seriously ill patients. Continuous Wave Doppler
(CW) records high speeds (5-20 m/s), however, it is impossible to accurately localize the area of the vascular bed under study.
systems —CDC
Color Doppler Imaging (CDI), which represents the next step in the development of ultrasound technology, makes it possible to easily locate a vessel and obtain color-coded information about the relative direction and speed of blood flow. It is accepted that red color shows the direction of blood movement towards the sensor, and blue - away from the sensor. Light colors mean high blood flow rates, saturated colors mean low ones.
A more accurate assessment of vascularity can be obtained using a modification of color Doppler energy mapping
— Color Doppler Energy (CDE), in which a color image of a vessel is obtained by recording the very fact of movement at a point in space (the presence of a Doppler frequency shift) and taking into account the energy of reflected signals. This type of scanning is more sensitive and increases the resolution of the method.
B-flow
is a new ultrasound technique in which, by subtracting two or four vectors along one scanning line, visualization of echo images from blood cells is achieved. At the same time, lateral noise that occurs when an ultrasonic beam passes through human tissue decreases or disappears. The technique allows you to simultaneously visualize the blood flow in the vessel, its lumen and walls, as well as the tissue surrounding the vessel. The study does not depend on the scanning angle; its use demonstrates the complete absence of artifacts.
3D mode
— further development of B-mode. A three-dimensional three-dimensional image is achieved by computer conversion of the signal obtained using a sensor with a changing plane of radiation. This method allows you to obtain a three-dimensional image of an organ and examine it in various projections. It turned out to be especially informative in the prenatal diagnosis of congenital anomalies of fetal development. Expert and high-class ultrasound devices have a 3D power Doppler or 3D ultrasound angiography mode. The device reconstructs a three-dimensional image of only the color part of the echogram, which characterizes the blood flow in the vessels. By changing the observation angle and rotating the three-dimensional image of the vessels, one gets an idea of the spatial location and shape of the vessels, which provides additional diagnostic information.
Duplex scanning
combines the capabilities of two-dimensional imaging in B-mode and spectral Doppler. This method allows you to simultaneously observe on the screen a grey-scale image of an organ and a Doppler frequency shift curve in real time.
Triplex scanning
— simultaneous real-time generation of a half-tone two-dimensional image, color-frequency flow information in a selected two-dimensional area, and a flow spectrogram.
Standard ultrasound examinations without the use of Doppler modes, if appropriate sensors are available, are possible on any of the devices listed above. Assessment of cardiovascular system parameters is carried out only in the presence of Doppler modes
, including continuous wave Doppler.
Next: features of ultrasound of the abdominal cavity and retroperitoneal space.
CONTENTS OF THE DOCUMENT
This document summarizes practical recommendations on how to perform Doppler ultrasound of the fetoplacental circulation. Of particular importance is the provision that the embryo and fetus should not be exposed to unnecessary harmful effects of ultrasound energy, especially in the early stages of pregnancy.
At these stages, Doppler ultrasonography should be performed when clinically indicated and using the lowest energy levels possible. ISUOG previously published guidelines for the use of Doppler ultrasound for fetal ultrasound examinations from 11 to 13+6 weeks of gestation (1).
When performing Doppler scanning, thermal index (TI) readings should not exceed 1 and exposure time should be kept to a minimum, usually no longer than 5–10 minutes and a maximum of 60 minutes (1). It is not the purpose of this guideline to define clinical indications, specify specific periods of pregnancy at which Doppler ultrasonography should be performed, discuss how diagnostic findings should be interpreted, or discuss the use of Doppler ultrasonography during fetal echocardiographic examinations.
The purpose of the manual is to describe pulsed wave Doppler ultrasound and its various modes such as spectral, color and energy, which are traditionally used in studies of blood circulation in the mother-placenta-fetus system. We will not describe the continuous wave Doppler method, since it is not usually used in obstetric ultrasound.
However, in cases where the fetus develops conditions that lead to very high flow rates (eg, aortic stenosis or tricuspid regurgitation), the method may be useful in accurately determining maximum flow rates without interference from aliasing artifact.
The methods and methods described in this manual have been selected to reduce measurement errors and improve reproducibility of results. However, in some cases they may not be applicable for some clinical conditions, as well as for research protocols.
Ultrasound Doppler of vessels

| Cost of Doppler ultrasound |
| from 2150 rub. |
Zaritskaya Valeria Valerievna
Ultrasound diagnostic doctor
MAKE AN APPOINTMENT
ASK A QUESTION TO AN EXPERT
Get a discount
Phone numbers for recording
+7 +7
Clinic address
Moscow, st. Vatutina, 13, bldg. 1 (metro Kuntsevskaya, metro Slavyansky Boulevard) Fili-Davydkovo, JSC Moscow
Operating mode
Fri.-Sat. from 8.00 to 21.00 Sunday from 8.00 to 18.00
Doppler study is one of the methods for studying blood flow in various vessels of the human body. Using a Doppler study, it is possible to determine the direction and speed of blood flow in the arteries and veins, the width of the lumen of the vessels, and also calculate the pressure inside the vessel. Doppler examination is performed using ultrasound.
How is a Doppler study performed?
Doppler examination is carried out using a special sensor that sends ultrasonic waves into the thickness of the body tissues and perceives the waves reflected from the tissues, which are later converted into an image using a computer. Vascular Doppler is possible due to the fact that blood cells moving in the vessels reflect ultrasonic waves, providing information about the direction and speed of blood movement inside the vessel.
Doppler examination of blood vessels is harmless, absolutely painless and does not require special preparation for the examination.
Doppler of neck and brain vessels
Doppler of cerebral vessels is an important method for diagnosing vascular diseases of the brain and spinal cord. Using Doppler of cerebral vessels, the quality of blood supply to the brain is assessed, and areas of narrowing or dilation of the arteries of the brain are identified. Doppler of cerebral vessels is recommended for people experiencing severe headaches, attacks of dizziness, fainting, and is also prescribed by a doctor if there is a risk of cerebrovascular accident (stroke), suspected aneurysm (expansion and thinning of a section of an artery) of a cerebral vessel, etc.
As a rule, during a session of Doppler diagnostics of cerebral vessels, a Doppler examination of the neck vessels supplying the brain (carotid arteries, vertebral arteries) is also performed.
Doppler of the heart and great vessels
Using Doppler ultrasound, it is possible not only to study blood flow in the vessels, but also to measure some indicators of heart function. Thus, using a Doppler study in combination with echocardiography (ultrasound of the heart), the direction and speed of blood movement in the chambers of the heart is determined. Doppler examination of the heart is recommended for children with suspected congenital heart defects, as well as for diagnosing other heart diseases.
Doppler examination of the vessels of the abdominal organs
Using Doppler ultrasound, it is possible to study large vessels of the abdominal cavity: the aorta, vessels supplying the intestines, spleen, liver, pancreas, kidneys, etc. Doppler of the vessels of the abdominal organs makes it possible to identify disturbances in the blood supply to the abdominal organs, for example, thrombosis of the mesenteric vessels (vessels feeding the intestines), which can lead to necrosis (death) of a section of the intestine, narrowing of the renal arteries, etc.
Doppler study of renal vessels
Doppler ultrasound of renal vessels is an important method for identifying the causes of some renal diseases, as well as arterial hypertension. Using Doppler ultrasound of the renal vessels, the width of the lumen of the renal arteries is determined, as well as the speed of blood movement through the renal vessels. Renal artery stenosis, detected by Doppler ultrasound of the renal vessels, is a narrowing of the lumen of the arteries that carry blood to the kidneys. Renal artery stenosis is the cause of arterial hypertension, which can occur even in childhood.
Doppler ultrasound of leg vessels
Leg vascular Doppler is usually prescribed when symptoms of diseases of the arteries or veins of the legs occur. Doppler ultrasound of the vessels of the legs is recommended for people who experience heaviness, pain in the legs or fatigue when walking, tingling sensations on the skin of the legs, increased sensitivity of the feet to cold, in case of ulcers appearing on the skin of the legs (long-term non-healing skin defects), as well as in the case of swelling in the legs, dilated veins visible under the skin (varicose veins) and in some other cases. No special preparation is required for Doppler ultrasound of leg vessels.
Vascular Doppler during pregnancy
Doppler ultrasound during pregnancy helps the doctor determine the quality of the blood supply to the developing fetus, find out the degree of patency and lumen of the fetal umbilical cord vessels, and also determine the fetal heartbeat. Doppler ultrasound is recommended for pregnant women suffering from hypertension, as well as eclampsia, in case of decreased motor activity of the fetus (rare movements), etc. see also Ultrasound during pregnancy.
A pregnant woman can independently determine the fetal heart rate using a special device called a fetal doppler. A fetal doppler is a small electronic device that listens to the fetal heartbeat and counts its heart rate.
RECOMMENDATIONS
What equipment is required for Doppler sonography when assessing fetoplacental circulation?
- The equipment must have color and spectral Doppler modes, displaying on the monitor screen the speed scale of blood flow or pulse repetition frequency (PRF), as well as the Doppler frequency of the sensor used (in MHz).
- Mechanical Index (MI) and Temperature Index (TI) should be displayed on the monitor screen.
- The ultrasound system should display a blood flow velocity curve (BVR) based on the maximum flow velocity, displaying the full spectrum of the Doppler wave.
- It should be possible to clearly delineate the CSC using a system of automatic or manual delineation (tracing) of the curve shape.
- The system must have software that allows the estimation of peak systolic velocity (PSV), end-diastolic velocity (EDV) and time-averaged maximum speed of the KSK and calculate conventional Doppler indices such as pulsatility index (PI) and resistance index (RI) as well as systolic-diastolic ratio (S/D). The KSK trace must display points that reflect the values that will be used for calculations to ensure the accuracy of the determined indices.
How can you optimize the accuracy of Doppler measurements?
Pulsed wave dopplerography
- Recording should be carried out during the absence of respiratory movements and motor activity of the fetus, and, if necessary, during the temporary holding of the mother’s breath.
- Color flow mapping is not mandatory, however it can be useful for identifying blood vessels of interest and determining the direction of blood flow.
- The optimal condition for insonation is complete coincidence of the direction of the ultrasound beam with the direction of blood flow. This provides ideal conditions for estimating absolute velocities and SSC spectra. Small deviations in the angle of insonation are acceptable.
An insonation angle of 10 degrees corresponds to a 2% error in velocity measurement, while an angle of 20 degrees corresponds to a 6% error. When the absolute velocity measurement is a clinically important parameter (eg, in the middle cerebral artery, MCA) and the resulting angle is greater than 20 degrees, angle correction can be used, but this itself may cause error.If the measured parameters do not improve with repeated attempts to optimize insonation, a record should be made in the study protocol indicating the angle of insonation, as well as information about whether an angle correction was used or whether the velocities were recorded without its correction.
- It is recommended to begin the study with a relatively large Doppler gate (sample volume) setting on the pulsed wave Doppler to ensure that the maximum velocity spectrum is recorded throughout the cardiac cycle. If pulsation in nearby vessels interferes with the waveform being studied, the control volume can be reduced to improve recording quality. It must be remembered that the control volume can only be reduced in height (in the vertical direction), but not in width.
- Similar to the gray scale scanning mode, the scanning depth and resolution of the Doppler signal (beam) can be optimized by adjusting the frequency (MHz) of the transducer.
- A frequency filter (wall filter), also called a “low velocity reject,” “wall motion filter,” or “high pass filter,” is used to eliminating noise caused by the movement of the vessel walls.
Traditionally, it should be set as low as possible (<50–60 Hz) to eliminate low-frequency noise from peripheral blood vessels. When using high frequency filter values, a false effect of missing end-diastolic velocity (EDV) may be created. (Fig. 4b). - High frequency filter values can be useful when assessing well-defined SSCs obtained from flows in structures such as the aortic and pulmonary outflow tracts. Setting the frequency filter to low values in these cases may be accompanied by the appearance of noise in the form of “flow artifacts” near the baseline or after the valve closes.
- The horizontal sweep speed of the Doppler spectrum must be fast enough to allow successive systolic-diastolic cycles to be separately identified. The most optimal is the simultaneous display of 4 to 6 (but not more than 8–10) complete cardiac cycles. For fetal heart rates between 110 and 150 bpm, a sweep speed of 50 to 100 mm/s is adequate.
- The pulse repetition rate (PRF) should be adjusted depending on the vessel being examined: low PRF values will allow visualization and accurate measurement of low-velocity blood flow; however, this will result in an aliasing artifact in the event of high-velocity regions. During Doppler measurements, the spectrum of the SSC should occupy at least 75% of the screen area (Fig. 3).
- Doppler measurements must be reproducible. If there are obvious discrepancies between measurement values, repeat measurements are recommended. Typically, the measurements closest to the expected ones are selected for the conclusion, with the exception of those obtained from spectra with low technical quality.
- In order to improve the quality of Doppler signal recording, it is necessary to carry out frequent real-time adjustments in gray scale mode or additionally use scanning in color Doppler mode. Then, when performing a CSC recording, after confirming in real time that the PW Doppler reference volume is positioned correctly, the two-dimensional (2D) and/or color Doppler (CD) modes should be frozen.
- You can confirm correct sample volume placement and optimize Doppler spectrum recording from a frozen 2D image by listening to the Doppler spectrum audio signal through audio speakers.
- The Doppler signal gain (Gain) must be adjusted so that the SSC spectrum can be clearly visualized, without artifacts in the background of the recording.
- It is recommended not to invert the flow direction on the monitor screen. When assessing the fetal heart and great vessels, it is very important to maintain the true direction of flow relative to the sensor when displayed in color in the Color Doppler mode and in the form of the direction of the FCS relative to the baseline in the Pulsed Wave Doppler mode. Traditionally, it is customary to map the blood flow directed to the ultrasound sensor in red, with the SSC spectrum located above the baseline, while the flow in the opposite direction (from the sensor) is displayed in blue and the SSC spectrum is located below the baseline.
Color Doppler mapping
- Compared to gray scale imaging, the use of color Doppler ultrasound increases the radiation power. The resolution of color Dopplerography increases with decreasing size of the “color window” (color box). It is necessary to pay close attention to the MI and TI indicators in view of the fact that their values change depending on the size and depth of the “color window”.
- Increasing the size of the “color window” also leads to an increase in signal processing time and, as a consequence, a decrease in the frame rate. The “window” should be as small as possible and include only the area of interest/area of interest.
- The velocity scale or pulse repetition rate should be adjusted to reflect the actual color velocity of the vessel being examined. When high PRF values are used, vessels with low blood flow velocities will not be displayed on the screen. When PRF values are used too low, an aliasing artifact appears that appears as inappropriate color coding of velocities, giving the appearance of bidirectional flow.
- As with gray scale imaging, the resolution and scanning depth of color Doppler are dependent on the ultrasound frequency. To optimize signals, the color Doppler frequency must be adjusted accordingly.
- Gain should be adjusted to prevent noise and artifacts, which appear as random color signals appearing in the background of the screen.
- A frequency filter must be adjusted to remove noise coming from the area being examined.
- The angle of insonation significantly affects the color Doppler image; it must be adjusted by optimizing the position of the ultrasound transducer according to the position of the blood vessel or area of interest. Energy and directional power Dopplerography
- All the same fundamental principles apply as for directional color Doppler.
- The angle of insonation has less influence on signal acquisition with power Doppler; however, when using this mode, the same image optimization techniques should be followed as for directional color Doppler.
- Aliasing artifact is not observed when using power Doppler PRF can lead to noise and artifacts.
- Gain should be reduced to prevent noise amplification (appears as a solid coloring of the background of the image).
Which technique should be used to evaluate Doppler waveforms of blood flow velocities in the uterine artery?
Using real-time color flow, the uterine artery is easily detected at the junction of the cervix and the body of the uterus. Measurement of Doppler blood flow velocities is usually performed in this position transabdominally (2, 3) or transvaginally (3–5). Taking into account that absolute values of blood flow velocities do not have fundamental clinical significance, a semi-quantitative assessment of BSC is usually performed.
Measurements should be taken separately for the right and left uterine arteries, and the presence of dicrotic notching on the uterine artery should be noted.
Assessment of the uterine arteries in the first trimester. (Fig. 1)
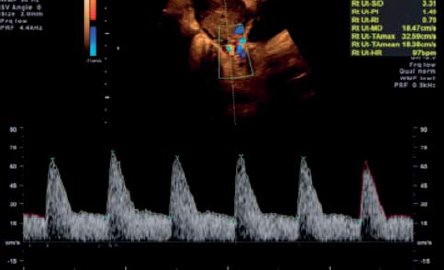
Rice. 1. Curve of blood flow velocity in the uterine artery, obtained through transabdominal access in the first trimester of pregnancy.
1. Transabdominal method
- The midsagittal plane of the section of the uterus is displayed transabdominally and the course of the cervical canal is visualized. It is preferable for the mother's bladder to be empty.
- The sensor is shifted laterally until the choroid plexus in the paracervical region begins to be visualized.
- The color Doppler mode is turned on and the uterine artery is visualized in the area of its turn in the cranial direction, where it begins to rise to the body of the uterus.
- Measurements are taken in the segment before the uterine artery begins to branch into the arcuate arteries.
- The same process is repeated on the opposite side.
2. Transvaginal method
- Transvaginally, the sensor is located in the anterior vaginal fornix. Next, a similar technique described for transabdominal access is used. The transducer is moved laterally until the paracervical choroid plexus is visualized, and the above steps are repeated in the same sequence as for the transabdominal method.
- Care must be taken to correctly differentiate the uterine arteries from the cervicovaginal (which have a cephalocaudal direction) or arcuate arteries. Velocities greater than 50 cm/s will be typical for the uterine arteries, which can be used to distinguish them from the arcuate arteries.
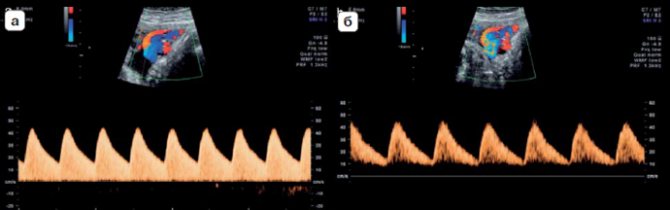
Evaluation of the uterine arteries in the second trimester (Fig. 2)
Rice. Fig. 2. Curves of blood flow velocities in the uterine artery obtained through transabdominal access in the second trimester of pregnancy. Normal (a) and pathological (b) spectrum; note the presence of a dicrotic notch (arrow) in the SSC spectrum (b).
1.Transabdominal method
- Transabdominally, the sensor is located longitudinally in the lower lateral quadrant of the abdomen with an inclination in the medial direction. To detect the uterine artery, which is visualized at the intersection with the external iliac artery, color Doppler ultrasound is used.
- The control volume of pulsed wave Doppler is located along the blood flow of the uterine artery 1 cm below the point of intersection of the two vessels. In those rare cases where the uterine artery bifurcates before its intersection with the external iliac artery, the control volume should be set to the segment up to its bifurcation.
- The same process is repeated for the uterine artery on the opposite side.
- As pregnancy progresses, the uterus usually rotates to the right. Therefore, the left uterine artery will not be defined as laterally as the right one.
2. Transvaginal method
- The woman must empty her bladder and is in the dorsal lithotomy position. The sensor should be located in the lateral vaginal vault, the uterine artery is determined using color Doppler ultrasound at the level of the internal os lateral to the cervix.
- The same process is repeated for the uterine artery on the opposite side. It must be remembered that the standard values of Doppler indices in the uterine arteries depend on the measurement method, therefore, for transabdominal (3) and transvaginal (5) access, appropriate standards must be used. In this case, the scanning technique should be similar to that which was used to obtain these standard values.
Note. In women with congenital uterine anomalies, assessment of uterine artery Doppler indices and their interpretation are not reliable since all studies were performed on women with (assumed) normal anatomy.
What technique should be used to evaluate Doppler waveforms of blood flow velocities in the umbilical artery?
There is a significant difference in Doppler measurements measured at the fetal end, the free loop, and the placental end of the umbilical cord (6). The highest resistance is seen at the fetal end, and thus null/reversed end-diastolic flow is most likely to be detected at this site first. Normative values of Doppler indices assessed at this location of the umbilical cord artery have been published in the literature (7, 8).
For the sake of simplicity and consistency, measurements should be taken at the level of the free loop of the umbilical cord. However, in cases of multiple pregnancies, and/or for comparison of repeated measurements over time, recording blood flows at “fixed sites”, for example, in the region of the fetal end, placental end or intra-abdominal segment, may be more reliable.
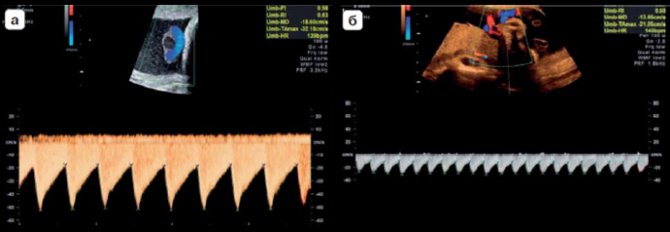
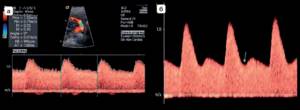
Rice. 3. Acceptable (a) and unacceptable (b) registration of blood flow velocity curves in the umbilical cord artery. In image (b), the blood flow spectrum is very shallow and the horizontal scan speed is too slow.
Rice. 4. Spectrum of umbilical cord artery flow velocity curves obtained from the same fetus at 4 min intervals showing (a) normal flow and (b) apparent very low diastolic flow and absence of flow signals near the baseline resulting from use inadequate setting of the frequency filter (which is set too high).
Depending on where the blood flow assessment was performed, appropriate guideline values must be used. In Fig. Figure 3 shows acceptable and unacceptable recording of blood flow velocity curves. Rice. 4 demonstrates the influence of the frequency filter on the appearance of the CSC.
Note. 1) In cases of multiple pregnancies, assessing blood flow in the umbilical cord artery can be difficult, due to the difficulty of determining which fetus belongs to a particular umbilical cord loop. In these cases, it is best to assess blood flow just distal to the umbilical cord's insertion into the fetal anterior abdominal wall.
However, vascular resistance in this area will be higher than at the level of the free loop or placental end, therefore it is necessary to use the appropriate standard values. 2) In the case of the presence of only two vessels in the umbilical cord, at any stage of pregnancy, the diameter of the single umbilical cord artery will be larger than in the presence of 2 arteries, and accordingly, vascular resistance will be lower (9).
What technique should be used to evaluate Doppler waveforms of blood flow velocities in the middle cerebral artery?
- A cross-section of the fetal head at the level of the thalamus and wings of the pterygoid should be drawn and the image magnified.
- To visualize the circle of Willis and the proximal part of the middle cerebral artery, the Color Doppler mode should be used (Fig. 5).
- The PW Doppler reference volume should be placed at the proximal third of the MCA in close proximity to its origin from the internal carotid artery (10) because systolic velocity decreases with increasing distance from the origin of this vessel.
- The angle between the ultrasound beam and the direction of blood flow should be kept as close to 0° as possible (Fig. 6).
- It is necessary to ensure that there is no excessive pressure on the fetal head.
- Simultaneous registration of at least 3, but not more than 10 consecutive cardiac cycles of CSC should be carried out. The highest point of the curve corresponds to the peak systolic velocity PSV (cm/s).
- PSV measurement can be done manually using callipers or using automatic tracing. The latter gives significantly lower average values compared to the first method (using callipers), but is closest to the published average values used in clinical practice (11). PI is usually calculated using automatic tracing, but manual delineation is also acceptable.
- Appropriate standards should be used to interpret the results. The measurement technique should be similar to that used to obtain standard values.

Rice. 5. Color Doppler mapping of the Circle of Willis.
Rice. 6. Acceptable recording of blood flow velocity curves in the middle cerebral artery. Notice the insonation angle is close to 0°.
What technique should be used to evaluate Doppler waveforms of fetal venous blood flow velocities?
Ductus venosus (Fig. 7 and 

- The ductus venosus (DV) connects the intra-abdominal segment of the umbilical vein with the superior portion of the inferior vena cava just below the diaphragm. This vessel can be visualized in gray scale (2D) mode in a midsagittal section of the fetal body or in an oblique cross section of the upper abdomen (12).
- At the narrow ostium of the ductus venosus, the circulatory system exhibits high-velocity flow, which helps to identify this vessel and determines the standard location for the control volume when performing Doppler measurements (13).
- Doppler measurements can best be obtained by scanning in a sagittal section from the anterioinferior aspect of the fetal abdomen, since the position of the reference volume in the isthmus can then be easily monitored. The sagittal approach through the chest can also be used, but requires greater skill from the operator. The oblique section provides acceptable access from an anterior or posterior position, allowing for adequate CVS appearance, but with less control over the angle of insonation and absolute velocities.
- In the early stages of pregnancy and in cases of pregnancy pathology, special attention should be paid to choosing an adequately small control volume of pulsed wave Doppler in order to achieve clear registration of low-velocity flows in the atrial systole phase.
- The spectrum of blood flow velocity curves usually has a three-phase appearance, but in rare observations, a biphasic or monophasic spectrum can also be recorded in healthy fetuses (14).
- During the second and third trimesters of pregnancy, relatively high blood flow velocities of 55 to 90 cm/s are recorded (15), but in early pregnancy these values are usually lower.
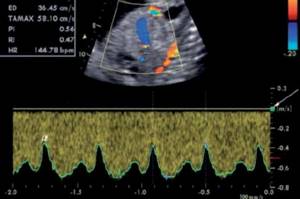
Rice. 7. Registration of the Doppler spectrum in the venous duct from the sagittal approach with the location of the control volume in the isthmus region without adjusting the angle. The low-pass filter (arrow) does not interfere with the registration of the a-wave (a), which is recorded significantly above the zero line. High horizontal scan speed allows detailed visualization of velocity changes during the cardiac cycle.

Rice. 8. Blood flow spectrum recorded in the ductus venosus, which shows increased pulsatility at 36 weeks (a). Interference, which is highly echogenic noise along the baseline, makes it difficult to confirm the presence of a reversal component during atrial systole (indicated by triangles). (b) repeated recording with slightly increased frequency filter values (arrow) improves the quality of the waveform recording and the clarity of visualization of reverse blood flow in the systole phase
What indicators to use?
Systole-diastolic ratio, RI and PI are three generally accepted indicators for describing arterial blood flow velocity curves. All three indicators are closely interrelated. PI shows a linear relationship with vascular resistance, in contrast to S/D and RI, which are characterized by a parabolic relationship with increasing vascular resistance (16).
In addition, PI does not lose its meaning in the case of zero or negative values of diastolic blood flow. PI is the most commonly used index in modern clinical practice.
By analogy, according to current literature, the pulsatility index for veins (PIV) is the most widely used indicator for assessing venous blood flow velocity curves (17). In some situations, the use of absolute rates may be preferable to semi-quantitative index measures.
Published in Wiley Online Library
Color Doppler mapping in the diagnosis of endometrial cancer

Ultrasound machine HS40
Top seller in high class.
21.5″ high-definition monitor, advanced cardio package (Strain+, Stress Echo), expert capabilities for 3D ultrasound in obstetrics and gynecology practice (STIC, Crystal Vue, 5D Follicle), high-density sensors.
Endometrial cancer is a fairly common pathology and ranks second among all malignant diseases of the female genital organs. Statistical data in recent years indicate a significant increase in the incidence of endometrial cancer - in our country the annual increase is approximately 6% per year [1]. Over the past 20 years, the incidence of endometrial cancer has doubled in Russia [2]. The maximum incidence of uterine cancer is observed at the age of 50-59 years [3,4].
In most cases, endometrial cancer is secondary and occurs against the background of precancerous diseases. G.M. Savelyev and V.N. Serov observed the transition of benign neoplastic processes to cancer in 79% of patients, Ya.V. Bokhman - 73% and T.V. Savinov - in 26% [5,3,6]. Precancerous diseases include atypical hyperplasia, adenomatous polyps, glandular cystic hyperplasia in menopause (especially recurrent) or developed against the background of neuroendocrine disorders [3,5,6]. The most common clinical sign of endometrial cancer is abnormal blood discharge from the genital tract. Despite the fact that endometrial cancer requires treatment as early as possible, it takes approximately 6 months from the appearance of the first signs of the disease to the final diagnosis [1].
The standard method for differential diagnosis of malignant and benign changes is histopathological examination of tissue obtained during separate diagnostic curettage of the uterus with hysteroscopic control. Today, the issue of exploring the possibilities of non-invasive tissue typing using color Doppler mapping, power Doppler, and pulsed Doppler is relevant. According to the literature, the systematic use of echography contributes to earlier diagnosis of endometrial cancer, increasing the incidence of stage I cancer by 50% and reducing the incidence of stage III-IV cancer by 1.5 times [7,8].
According to most authors, the use of complex ultrasound examination with analysis of blood flow velocity curves is a highly informative method for non-invasive diagnosis of endometrial carcinoma, since in the vast majority of cases of the disease there are pathological blood flow velocity curves characteristic of the vascular network with a low level of peripheral resistance. The resistance and pulsation indices made it possible to prove the absence of the muscular membrane in the wall of arterial vessels in the neovascularization basin during malignant tumor growth. The resistance index (RI) for endometrial carcinoma is 0.42+0.02, whereas normally, with endometrial atrophy and simple hyperplasia, endometrial blood flow is not recorded [9,10-14]. However, ultrasound studies that reveal the capabilities of color Doppler sonography in diagnosing endometrial cancer are extremely insufficient.
The purpose of the work is to study the possibilities of complex ultrasound examination using color Doppler mapping, power Doppler, pulsed Doppler in the differential diagnosis of benign and malignant endometrial pathology in determining the stage, degree of differentiation and depth of invasion of the tumor process into the myometrium.
Materials and methods
We examined 40 pre- and postmenopausal patients with endometrial pathology. A standard algorithm for examining this group of patients was used. The diagnosis was verified by morphological examination of the removed specimen. 17 (42.5%) cases of hyperplastic and 23 (57.5%) cases of malignant endometrial processes were found. The average age of patients with benign pathology was 46.8±8.1 years, with endometrial cancer - 58.5±7 years. The data of the morphological study of patients are presented in table. 1.
Table 1
. Morphological study of patients with endometrial pathology.
| Morphological form | Quantity | % |
| Hyperplastic processes | 17 | 42,5 |
| Glandular cystic hyperplasia Glandular fibrous polyps Atrophic endometrium Atypical hyperplasia | 9 4 1 3 | 22,5 10 2,5 7,5 |
| Malignant pathology | 23 | 57,5 |
| Adenocarcinoma Squamous cell carcinoma Adenoacanthoma Combination of adenocarcinoma and endometrial stromal sarcoma | 17 3 2 1 | 42,5 7,5 5 2,5 |
| Total | 40 | 40 |
In 10 (58.8%) patients with hyperplastic processes and in 14 (60.9%) patients with endometrial adenocarcinoma, concomitant small uterine fibroids were observed (5-9 weeks of pregnancy). Long-term existence of uterine fibroids (6-10 or more than 10 years) was noted in all patients with adenocarcinoma.
Ultrasound examination in combination with color Doppler mapping, power Doppler and pulsed Doppler was performed on all patients using modern ultrasound machines using transabdominal (convex sensor with a frequency of 3.5 MHz) and transvaginal (convex sensor with a frequency of 6.5 and 7 MHz) access. Ultrasound examination assessed the size of the uterus, size, structure, and condition of the uterine cavity and ovaries. Doppler analysis included determination of: the nature of blood flow (arterial or venous), the number of color signals from vessels in each tumor, the localization of intratumoral blood flow (central or peripheral), the lowest and average resistance index (RImin and RImed) in the uterine, arcuate and tumor vessels, the maximum speed of arterial (VAmax) and venous blood flow (VVmax).
To eliminate subjectivity in assessing the intensity of intratumoral blood flow, we have proposed a scale. In 5-6 still frames, the number of color signals from the vessels of the neoplasm was recorded:
- “poor” intratumoral blood flow was represented by single color signals from vessels - no more than 5;
- moderately expressed - 5-10 color signals;
- intense, pronounced blood flow - more than 10 color signals from vessels.
For the uterine arteries, a frequency filter of 100 and 50 Hz was used, for the arcuate and intratumoral vessels, with a Doppler beam “trial volume” size of 4 and 2 mm, respectively.
Results and its discussion
Group 1 - hyperplastic processes of the endometrium (n=17)
. Clinically, benign endometrial pathology was manifested by menstrual cycle disorders such as menometrorrhagia, and grade I-II anemia in 47.1% of patients. Their examination revealed an increase in the thickness of the M-echo with benign endometrial pathology on average - 13.8 mm (range 6-23 mm). With transvaginal echography, glandular cystic hyperplasia was defined as the formation of increased echogenicity, a homogeneous spongy structure with multiple point anechoic inclusions and an acoustic enhancement effect. With atypical hyperplasia, a heterogeneous hyperechoic structure was found in the uterine cavity. Polyps were noted as oval or round hyperechoic formations, deforming the uterine cavity, with a small amount of fluid. In benign endometrial neoplasms, a clear and smooth outer contour of the M-echo was detected.
Color Dopplerography did not register intratumoral blood flow in 23.5% of patients: with atrophic endometrium and in 3 cases of glandular cystic hyperplasia. In 76.5% of patients, peripheral blood flow of varying intensity was found with average values of the resistance index. In glandular cystic hyperplasia, single color signals were noted from vessels located along the periphery, with medium and high values of the resistance index. In fibroglandular polyps, moderately pronounced venous and arterial peripheral blood flow with average values of peripheral vascular resistance was visualized. In atypical hyperplasia, intense central and peripheral intratumoral blood flow with an average level of vascular resistance was recorded.
The minimum resistance index (RImin) for endometrial hyperplastic processes was 0.56+0.05; the maximum speed of arterial blood flow is 9.3 cm/s (fluctuations 5-13 cm/s), the maximum speed of venous blood flow is 5 cm/s (fluctuations 3-5 cm/s).
Group 2 - malignant pathology of the endometrium (n=23)
. Malignant transformation of the endometrium in most cases was accompanied by postmenopausal bleeding and varying degrees of anemia in 73.9% of patients.
The cancer stage was determined according to the International Classification of Cancer of the Endometrium (FIGO, 1988). A comparison of stage and histotype is presented in Table. 2.
table 2
. Comparison of histotype and stage of endometrial cancer.
| Stage | Adenocarcinoma | Other* | Total | |
| highly differentiated | moderately differentiated | |||
| Ia | 4 | — | 1 | 5 |
| Ib | 4 | 4 | 4 | 12 |
| Ic | — | — | — | — |
| II | — | 2 | 1 | 3 |
| III | — | 2 | — | 2 |
| IVc | — | 1 | — | 1 |
| Total: | 8 | 9 | 6 | 23 |
Note. * Adenoacanthoma stages Ia, Ib - 2 cases, squamous cell carcinoma stage Ib - 3 cases, combination of adenocarcinoma and endometrial stromal sarcoma stage II - 1 case.
In our study, the degree of tumor differentiation correlated with the stage of the disease: a highly differentiated process was limited to the body of the uterus, with moderately differentiated adenocarcinoma stages II, III and IV (tumor spread beyond the organ) were noted. An examination of patients with suspected endometrial cancer revealed an increase in the thickness of the M-echo to 18.1 mm (range 7-38 mm). At stage Ia - the thickness of the M-echo was 11.6 mm (fluctuations 7-20 mm), at stage Ib - 16.5 mm (fluctuations 7-38 mm), at stage II - 31 mm (fluctuations 27-33 mm) , at stage III - 17.5 mm (fluctuations 16-19 mm), at stage IV - 29 mm.
Ultrasound signs of malignant pathology of the endometrium were: heterogeneity of the internal structure of the formation, higher echogenicity compared to the myometrium, increased sound conductivity of the tissue, an uneven, “corroded” contour penetrating into the myometrium to varying depths, the presence of a hypoechoic rim around the tumor.
In 30.4% of patients with endometrial carcinoma, transvaginal echography revealed local hyperechoic formations of a heterogeneous internal structure with predominant invasion in a certain direction of one of the uterine walls or localization in the fundus or one of the tubal angles. A morphological study revealed an exophytic form of tumor growth of stage I. In the remaining 69.6% of clinical observations, an endophytic form of growth with uniform invasion into the myometrium was noted. These patients were found to have uneven, “eaten away” contours of the tumor, penetrating into the myometrium to varying depths, and an erased boundary between the tumor and the myometrium. Tumor necrosis with deformation of the uterine cavity and the presence of a certain amount of fluid were detected at stages III and IV of the process.
Endometrial neovascularization occurred in 91.3% (21) of patients. Of these, “poor” and moderately expressed blood flow with low resistance index numbers was observed in 13% of cases of well-differentiated stage Ia adenocarcinoma. This type of neovascularization is observed in exophytic forms of tumor growth.
Intense intratumoral blood flow was detected in 78.3% of patients. Color Dopplerography revealed a scattered type of blood supply to the uterus along the vascular bundle, rich vascularization of the myometrium with medium and low levels of vascular resistance, as well as neovascularization of the endometrium with a “mosaic” form of mapping and a low level of peripheral resistance of newly formed vessels. Of these, in 21.7% of cases, a predominantly venous type of intratumoral blood flow was noted in the area of neovascularization and with a maximum velocity of venous blood flow of 8.3 cm/s (fluctuations 4-13 cm/s).
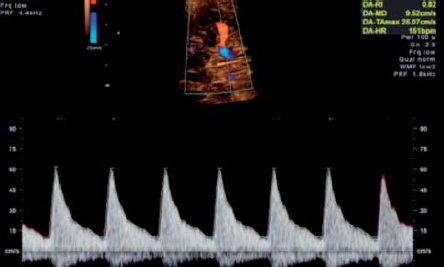
The intensity of blood flow depended on the form of tumor growth: in the exophytic form, an intratumoral type of neovascularization was noted, in the endophytic form, an intense intra- and peritumoral type of blood flow, rich vascularization of the myometrium (Fig. 1).
Rice. 1.
Intratumoral type of blood flow in endometrial cancer.
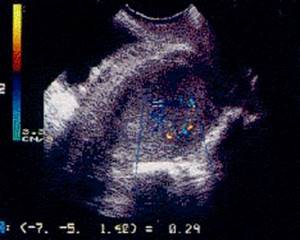
A)
Intra- and peritumoral.

b)
Intratumoral.
Although there was a direct correlation between the severity of tumor blood flow and the stage, as well as the degree of differentiation, the zone of neovascularization corresponded to a significantly higher stage of the process.
RImin in the neovascularization basin was 0.36+0.05, the maximum arterial blood flow velocity was 10.2 cm/s (fluctuations 4-22 cm/s). Different histotypes of endometrial cancer had identical intratumoral blood flow and low resistance index values.
Color Doppler ultrasound did not register neovascularization of the pathological process in 8.7% of cases. The reason for this could be the removal of a small tumor as a result of preliminary diagnostic curettage of the uterine cavity - in case of stage Ia adenoacanthoma and the occurrence of a malignant process against the background of endometrial atrophy in case of well-differentiated stage Ia adenocarcinoma.
In table Table 3 shows a comparative description of Doppler parameters in benign and malignant endometrial pathologies.
Table 3
. Hemodynamics in benign and malignant pathology of the endometrium.
| Group 1 Endometrial hyperplasia, n=17 | Group II Endometrial cancer, n=23 | |
| Intratumoral vessels | ||
| Hemodynamic indicator | No or peripheral blood flow | Intense blood flow - central and peripheral |
| RImin | 0,56+0,05 | 0.36+0.05 (p |
| RImed | 0,60+0,08 | 0,43+0,07 |
| Range | 0,50-0,73 | 0,27-0,65 |
| VAmax | 9.3 cm/s | 10.2 cm/s |
| Range | 5-13 | 4-22 cm/s |
| VVmax | 5 cm/s | 8.3 cm/s |
| Range | 3-5 | 4-13 |
| Arcuate arteries | ||
| RImin | 0,61+0,07 | 0,55+0,1 |
| RImed | 0,69+0,08 | 0,61+0,1 |
| Range | 0,50-0,88 | 0,38-0,83 |
| VAmax | 18 cm/s | 15.4 cm/s |
| Range | 9-28 | 3-34 |
| Uterine arteries | ||
| RImed | 0,82+0,07 | 0,79+0,07 |
conclusions
In benign processes of the endometrium, peripheral intratumoral blood flow is detected with average values of the resistance index or the absence of blood flow. Malignant transformation of the endometrium is characterized by the presence of neovascularization of the tumor: intense central and peripheral tumor blood flow, chaotic arrangement of vessels with a low level of peripheral vascular resistance.
The difference in the minimum resistance indices of intratumoral vessels in benign and malignant endometrial pathologies is statistically significant (RImin 0.56±0.05 and 0.36±0.05, respectively, рmin = 0.36±0.05 in our work was 91.3 %, specificity - 89.5%.
There were no significant differences in the levels of maximum arterial blood flow velocity (9.3 cm/s and 10.2 cm/s, respectively) and maximum venous blood flow velocity (5 cm/s and 8.3 cm/s, respectively) in both groups of patients.
Ultrasound examination using color Doppler mapping, power Doppler, and pulsed Doppler does not allow assessing the tumor histotype before surgery. But the level of vascularization of the process revealed using color Doppler sonography makes it possible to predict the rate of growth of the detected neoplasm.
Thus, a comprehensive ultrasound examination using color and power Doppler, pulsed Doppler is a highly informative method of non-invasive diagnostics. The results obtained indicate the high accuracy of the method in the differential diagnosis of benign and malignant endometrial pathology.
Literature
- Ashrafyan L.A. Standardized diagnosis of endometrial cancer: Abstract. dis. doc. honey. Sci. - M., 1989. - 40 p.
- Maksimova N.A. Some aspects of ultrasound diagnosis of endometrial cancer // Ultrasound. diag. obstetrician, gynecological, pediatrician. — 1999.-N3. — P. 196-201.
- Bokhman Y.V. Guide to gynecological oncology. - Medicine: L., 1989. - 463 p.
- Demidov V.N., Krasikova S.P. Endometrial cancer - possible ways to prevent it. Ultrasound examination / Clinical lectures on ultrasound diagnostics in obstetrics, gynecology and perinatology. - M., 1994.-S. 66-78.
- Savelyeva G.M., Serov V.N. Endometrial precancer. - M.: Medicine, 1980.-168 p.
- Savinova T.V. Early stage endometrial cancer // Obstetrics. and gin. - 1988. - N5. -WITH. 19-24.
- Kharchenko N.V. Possibilities of echography in primary and clarifying diagnostics of endometrial cancer / Abstract. dis. Ph.D. honey. Sci. - M., 1996. - 22 p.
- Demidov V.N., Gus A.Y. Ultrasound diagnosis of hyperplastic and tumor processes of the endometrium // Ed. V.V. Mitkova, M.V. Medvedev. Clinical guide to ultrasound diagnostics, 3 volumes - Vidar: M., 1997.-P. 120-131.
- Rakits S., Markovich A., Dyukits M. et al. Diagnosis of endometrial cancer using transvaginal color Doppler ultrasonography // Sonoace international: trans. English — Russian version, 1996.-N1. — P. 16 22.
- Teregulova L.E. Transvaginal echography using color Doppler mapping in patients with endometrial cancer // Ultrasound. diag., 1996. - N4. — P. 21-23.
- Bourne TH, Crayford T, Hanapson J, Reynolds K et al. Transvaginal color Doppler ultrasonography for the diagnosis of uterine cancer // Ultrasound Obstet. Gynecol., 1992, vol. 2, Suppl. 1, p. 75.
- Hata K., Hata T., Kitao M. Intratumoral blood flow analysis in endometrial cancer: does it differ among individual tumor characteristics? // Gynecol-Oncol., 1996, June; 61(3): 341-344.
- Kurjak A., Shalan H., Sosic A., Benic S. et al. Endometrial carcinoma in postmenopausal women: evaluation by transvaginal color Doppler ultrasonography // Am. J. Obstet. Gynecol., 1993, v. 169, p. 1597-1603.
- Olaya FJ, Dualde D, Garcia E, Vidal P, Labrador T., Martinez F, Gordo G. Transvaginal sonography in endometrial carcinoma: preoperative assessment of the depth of myometrial invasion in 50 cases // Eur. J. Radiol., 1998, Feb., 26(3), p. 274-279.
Ultrasound machine HS40
Top seller in high class.
21.5″ high-definition monitor, advanced cardio package (Strain+, Stress Echo), expert capabilities for 3D ultrasound in obstetrics and gynecology practice (STIC, Crystal Vue, 5D Follicle), high-density sensors.
Literature
1. Salvesen K, Lees C, Abramowicz J, Brezinka C, Ter Har G, Marsal K. ISUOG statement on the safe use of Doppler in the 11 to 13+6-week fetal ultrasound examination. Ultrasound Obstet Gynecol 2011; 37:628.
2. Aquilina J, Barnett A, Thompson O, Harrington K. Comprehensive analysis of uterine artery flow velocity waveforms for the prediction of pre-eclampsia. Ultrasound Obstet Gynecol 2000; 16: 163–170.
3. Gomez O, Figueras F, Fern{andez S, Bennasar M, Martinez JM, Puerto B, Gratacos E. Reference ranges for uterine artery mean pulsatility index at 11–41 weeks of gestation. Ultrasound Obstet Gynecol 2008; 32: 128–132.
4. Jurkovic D, Jauniaux E, Kurjak A, Hustin J, Campbell S, Nicolaides KH. Transvaginal color Doppler assessment of the uteroplacental circulation in early pregnancy. Obstet Gynecol 1991; 77:365–369.
5. Papageorghiou AT, Yu CK, Bindra R, Pandis G, Nicolaides KH; Fetal Medicine Foundation Second Trimester Screening Group. Multicenter screening for pre-eclampsia and fetal growth restriction by transvaginal uterine artery Doppler at 23 weeks of gestation. Ultrasound Obstet Gynecol 2001; 18:441–449.
6. Khare M, Paul S, Konje J. Variation in Doppler indices along the length of the cord from the intraabdominal to the placental insertion. Acta Obstet Gynecol Scand 2006; 85:922–928.
7. Acharya G, Wilsgaard T, Berntsen G, Maltau J, Kiserud T. Reference ranges for serial measurements of blood velocity and pulsatility index at the intra-abdominal portion, and fetal and placental ends of the umbilical artery. Ultrasound Obstet Gynecol 2005; 26: 162–169.
8. Acharya G, Wilsgaard T, Berntsen G, Maltau J, Kiserud T. Reference ranges for serial measurements of umbilical artery Doppler indices in the second half of pregnancy. Am J Obstet Gynecol 2005; 192:937–944.
9. Sepulveda W, Peek MJ, Hassan J, Hollingsworth J. Umbilical vein to artery ratio in fetuses with single umbilical artery. Ultrasound Obstet Gynecol 1996; 8:23–26.
10. Mari G for the collaborative group for Doppler assessment. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red-cell alloimmunization. N Engl J Med 2000; 342:9–14.
11. Patterson TM, Alexander A, Szychowski JM, Owen J. Middle cerebral artery median peak systolic velocity validation: effect of measurement technique. Am J Perinatol 2010; 27: 625–630.
12. Kiserud T, Eik-Nes SH, Blaas HG, Hellevik LR. Ultrasonographic velocimetry of the fetal ductus venosus. Lancet 1991; 338:1412–1414.
13. Acharya G, Kiserud T. Pulsations of the ductus venosus blood velocity and diameter are more pronounced at the outlet than at the inlet. Eur J Obstet Gynecol Reprod Biol 1999; 84: 149–154.
14. Kiserud T. Hemodynamics of the ductus venosus. Eur J Obstet Gynecol Reprod Biol 1999; 84: 139–147.
15. Kessler J, Rasmussen S, Hanson M, Kiserud T. Longitudinal reference ranges for ductus venosus flow velocities and waveform indices. Ultrasound Obstet Gynecol 2006; 28:890–898.
16. Ochi H, Suginami H, Matsubara K, Taniguchi H, Yano J, Matsuura S. Micro-bead embolization of uterine spiral arteries and uterine arterial flow velocity waveforms in the pregnant woman. Ultrasound Obstet Gynecol 1995; 6:272–276.
17. Hecher K, Campbell S, Snijders R, Nicolaides K. Reference ranges for fetal venous and atrioventricular blood flow parameters. Ultrasound Obstet Gynecol 1994; 4: 381–390.
www.isuog.org
- Views: 28995
- Comments: