Magnetic resonance imaging (MRI) in St. Petersburg
Localization of the pathological focus with MRI of the brain begins with determining the location of the lesion in relation to the tentorium of the cerebellum. Therefore, formations above the tentorium are classified as supratentorial, and everything below is classified as infratentorial.
MRI of the brain. Midsagittal section. tentorium cerebellum (arrow).
Above the tentorium are the cerebral hemispheres. Each hemisphere of the brain consists of four lobes - frontal, parietal, occipital and temporal. If the pathology is located in the hemisphere, then it is necessary to decide which lobe it belongs to. To do this, you first need to find the grooves that serve as the boundaries of the lobes. The central sulcus (sulc.centralis) is better visible in the sagittal plane. It is located in the middle between the parallel precentral and postcentral sulci. There are many options for the structure and course of the furrow. Usually it has a significant extent and goes in the anterior-inferior direction from the interhemispheric fissure to the Sylvian fissure, which it does not always reach. The lower end of the furrow either continues in its main direction or bends back. The central sulcus may be interrupted along the way. In the transverse plane on the upper sections the groove has the greatest extent, reaching almost to the interhemispheric fissure. The lower the cut, the shorter the central groove on it. At the level of the lateral ventricles it is barely visible. The central sulcus separates the frontal and parietal lobes.
MRI of the brain. Lateral sagittal section. Central sulcus (arrow).
MRI of the brain. Axial slice. Central sulcus (arrows).
MRI of the brain. Axial section at the level of the roof of the lateral ventricles. Central sulcus (arrows).
MRI of the brain. Borders of the frontal and parietal lobes in the axial plane.
Another important groove is the Sylvian fissure (fissura cerebri lateralis). On sagittal sections it goes from bottom to top in the anteroposterior direction (Fig. 32). In the axial plane, the Sylvian fissure itself also deviates backward, while its branches are directed perpendicularly towards the interhemispheric fissure. The Sylvian fissure separates the frontal and parietal lobes from the temporal lobe.
MRI of the brain. Lateral sagittal section. Sylvian fissure (arrows).
MRI of the brain. Axial section at the level of the third ventricle. Sylvian fissure (arrows).
MRI of the brain. Borders of the frontal, parietal, temporal and occipital lobes on a sagittal section.
To delimit the parietal lobe, you also need to find the parieto-occipital sulcus (sulc. parietooccipitalis). This groove in the sagittal plane can be traced on the median and medial sections. It extends from the surface of the brain downwards, has a considerable extent and is often segmented. In the transverse plane, the parieto-occipital sulcus extends almost perpendicular to the interhemispheric fissure (Fig. 36) and gives off many small branches. Thus, the boundaries of the parietal lobe are with the frontal lobe - the central sulcus, with the occipital - the parieto-occipital sulcus, with the temporal - the Sylvian fissure and the superior temporal sulcus (angular gyrus).
MRI of the brain. Medial sagittal section. Parieto-occipital sulcus (arrow).
MRI of the brain. Axial slice. Parieto-occipital sulcus (arrow).
MRI of the brain. Borders of the parietal lobe on the medial sagittal section.
The next important dividing groove is the collateral groove (sulc.collateralis). On sagittal sections, it is visible as the inferolateral border of the parahippocampal gyrus, in the region of the pole of the temporal lobe (Fig. 38). It is easier to see in the axial plane in sections at the level of the midbrain (Fig. 39). When the axial plane of the slices is tilted backward, it is visible simultaneously with the temporo-occipital groove. The temporo-occipital groove (sulc. temporooccipitalis) on lateral sagittal sections runs sinuously backward along the border of the brain with the temporal bone and then bends upward (Fig. 40). On axial sections at the level of the Varoliev bridge, it is located in the anteroposterior direction. Thus, the border of the temporal lobe (Fig. 41) with the frontal and parietal lobes is the Sylvian fissure, with the occipital lobe - the temporo-occipital sulcus and the collateral sulcus.
MRI of the brain. Sagittal section. Collateral groove (arrow).
MRI of the brain. Axial slice. Collateral groove (arrows).
MRI of the brain. Axial section at the level of the Varoliev bridge. Temporo-occipital sulcus (arrows).
MRI of the brain. Axial section at the level of the cerebral peduncles. Borders of the temporal lobe.
To determine the boundaries of the occipital lobe, we already have all the landmarks. The border with the parietal lobe is the medially located parieto-occipital sulcus, and the border with the temporal lobe is the laterally located temporo-occipital sulcus.
MRI of the brain. Coronal section. Border sulci (SPO - parieto-occipital sulcus, STO - temporo-occipital sulcus, SCol - collateral sulcus).
MRI of the brain. Borders of the occipital lobe on the medial sagittal section.
Usually localization by lobes is sufficient to describe hemispheric pathologies. In some cases, when reference to gyri or functional areas is required, we recommend using the appropriate atlases (A.V. Kholin, 2005). With centrally (axially) located space-occupying formations, the ventricles of the brain and the subcortical (basal) nuclei located around them may be involved. The optic thalamus, hypothalamus, subthalamus, and epithalamus belong to the diencephalon, a component of the brain stem.
MRI of the brain. Axial slice. Lateral ventricles and subcortical nuclei (NC - caudate nucleus, NL - lenticular nucleus, Th - thalamus optic). Parts of the brainstem (lower midbrain, pons, and medulla oblongata) and the cerebellum are located infratentorially.
The midbrain only partially occupies the supratentorial space; a significant part of it passes through the hole in the tentorium into the posterior cranium. hole. The paired legs of the brain and roof (tectum) are always clearly visible from behind. The roof of the midbrain lies posterior to the aqueduct and consists of the quadrigeminal plate.
MRI of the brain. Midsagittal section. Brain stem (V3 - third ventricle, V4 - fourth ventricle, Q - plate quadrigeminal, Mes - midbrain, P - pons, C - cerebellum, M - medulla oblongata).
The boundary between the midbrain and the pons is the superior sulcus, and the border with the medulla oblongata is the inferior sulcus of the pons. The bridge has a characteristic protruding front part. The posterior surface of the pons is a continuation of the medulla oblongata. At the upper border of the bridge between its abdomen and the middle cerebellar peduncle, the trigeminal nerves (n. trigeminus, V pair) begin. They are clearly visible on transverse MR sections, as they run horizontally forward and have a thickness of about 5 mm. The trigeminal nerve is divided into 3 branches - optic (1), maxillary (2) and mandibular (3). They all go forward into Meckel's cavity to the trigeminal ganglion. From here the 3rd branch goes down through the foramen ovale, and the 1st and 2nd branches go through the cavernous sinus, along its lateral wall. Then, branch 1 enters the orbit through the superior foramen, and branch 2 exits the cranial cavity through the foramen rotundum. The III, IV and VI pairs of cranial nerves, which provide movement of the eyeball, are usually not visualized on MRI scans.
MRI of the brain. Axial slice. Trigeminal nerves (arrow).
The facial nerve (n. facialis, VII pair) and the vestibular-cochlear nerve (n. vestibulocochlearis, VIII pair) exit their trunk together, the facial nerve is slightly more medial, and go in one bundle, crossing the pontocerebellar cistern, and go into the internal auditory opening temporal bone. In the internal auditory canal, the vestibular branch runs in the posterior superior and inferior quadrants, the cochlear branch in the inferior, and the facial nerve in the anterior superior. The VII nerve enters the labyrinth (labyrinthine segment), runs inside the temporal bone to the geniculate body, turns back and passes under the lateral semicircular canal (tympanic segment) and exits the temporal bone through the stylomastoid foramen (foramen stylomastoideum). Next, the nerve goes to the salivary gland, where it divides into terminal branches. On MRI scans in sections 3-5 mm thick, the VII and VIII nerves are not separated and are designated as the auditory nerve. With thinner sections, the course of each nerve can be visualized separately.
MRI of the brain. Axial slice. Auditory nerve.
The medulla oblongata begins from the lower border of the pons. At the level of the foramen magnum it passes into the spinal cord. From it depart from the IX to XII pairs of cranial nerves, of which the initial part of the hypoglossal nerve (n. hypoglossus, XII pair) and, in the form of a single complex, IX, X, XI pairs are sometimes visible on transverse MRI. The IV ventricle runs from the aqueduct above to the foramen of Majendie below. It is located between the brainstem anteriorly and the velum and cerebellar peduncles posteriorly. Posterior to the pons and medulla oblongata is the cerebellum. It is connected to the brain stem by the superior, middle and inferior cerebellar peduncles. The cerebellum consists of a midline vermis and paired hemispheres.
MRI of the brain. Axial slice. Cerebellum (CV - cerebellar vermis, CH - cerebellar hemisphere).
MRI in St. Petersburg, carried out by us, always clearly indicates the localization of the lesion in the report, which is necessary for comparison with the clinic and deciding on the possibility and scope of the operation.
Leave feedback.
MRI in St. Petersburg USA
Vascular MRI (angiography) in Kemerovo. Cost, sign up for an MRI in Magnesia
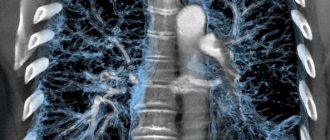
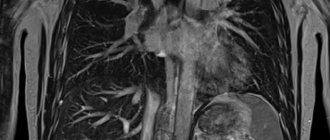
Magnetic resonance angiography (MRI of vessels) is one of the most reliable and informative methods of modern diagnostics and allows you to clearly visualize vascular structures, without the use of a contrast agent and without radiation exposure.
IMPORTANT: in Magnesia we conduct a comprehensive study of arteries and veins together, without dividing the study of the vascular bed into arteriography and venography!
Most often, MR angiography is used to diagnose pathologies of the circulatory system of the brain.
MRI of brain vessels determines the intensity of blood flow in the vessels; helps to detect pathological changes at an early stage, determine treatment tactics, and track the dynamics of changes over time.
Doctors prescribe MRI angiography of the arteries and veins of the brain to identify the causes of cerebral circulatory failure. A common cause of headaches, dizziness, visual disturbances, memory loss and other neurological symptoms can be vertebrobasilar insufficiency (narrowing of the carotid or vertebral arteries).
Indications for MR angiography of the brain
The study is indicated if there is a history or suspicion of the following diagnoses:
- arteriovenous malformation (AVM), vascular malformation;
It is a congenital anomaly of the development of the vascular system of the brain and consists of tangles of various shapes and sizes, formed as a result of the random interweaving of pathological vessels.
- neurovascular (vasoneural) conflict (NVC);
This is compression or deformation of the cranial nerve root near the brain stem. The pathology, according to statistics, is more common in women; the majority of cases are people over 50 years of age.
- aneurysm;
A cerebral aneurysm, or intracranial aneurysm, is an expansion of an artery in a local area caused by damage to its wall. It grows quickly, filling with blood. In this case, expansion of the formation is observed, a noticeable bulge appears.
- increased thrombus formation;
- neoplasms (tumors).
You should also be alarmed if your memory and attention are deteriorating, or you often feel dizzy or sore. This may be a sign of pathological conditions.
Angiography may also be prescribed if surgical intervention is necessary in the area of vessels and veins. MRI angiography is often performed after treatment to assess the dynamics.
MR angiography of cerebral vessels without examining the brain itself is not very informative.
For example, if a blood flow disorder is detected, the cause will most likely not be identified based only on an angiographic study. Impaired blood flow can be caused by external causes, such as tumors, developmental abnormalities, etc. And vice versa - it is important to evaluate not only the pathological process in the vascular bed, but also how this affects the substance of the brain.
Indications for MRI of the head and angiography of arteries, veins and venous sinuses:
- strokes;
- traumatic brain injuries;
- fainting;
- suspicion of vascular abnormalities;
- noise in ears;
- hearing and vision impairment;
- dizziness, migraines, unreasonable nausea and vomiting;
- loss of body coordination;
- asymmetric pain, spasm or numbness of one half of the face;
- examination to detect neoplasms, benign and malignant tumors;
- determining the stage of tumor development;
- detection of metastases and determination of the area affected by them;
- assessment of the effectiveness of surgery and chemotherapy for brain tumors.
Most often, these symptoms can be caused by a short-term decrease in cerebral blood flow. Dizziness usually occurs as a result of impaired blood supply to the brain or in cases where the brain substance itself is damaged.
Severe and prolonged headaches on one side of the head (less often on both), which are accompanied by symptoms such as feeling unwell, nausea, irritation, and sometimes vomiting, may indicate a migraine or brain diseases that have similar symptoms.
What examination should be performed for such symptoms as: headache, dizziness, darkening of the eyes and migraines?
Firstly, the examination should be as complete as possible so that the doctor can create the best plan to solve the problem and cause. If an MRI of the brain with angiography of the vessels does not provide the necessary picture of the problem, then an MRI of the cervical spine with angiography of the vessels of the neck may be prescribed, since with osteochondrosis of the neck, the headache appears in both the neck and the back of the head, and then moves to one of the halves heads. The pain may vary in intensity and nature, and may be accompanied by dizziness and nausea. In our center, for such cases, we provide comprehensive studies of the causes of headaches, dizziness, migraines, pressure changes, as well as darkening of the eyes.
How is vascular MRI angiography performed?
Magnetic resonance imaging of vessels in angiography mode does not feel different from a standard study.
The patient changes into clothes without metal inserts or into a disposable uniform.
Advantages of MR angiography as a method
- High information content and accuracy of the method;
- Safety of the study;
- Detection of diseases (organic changes) in the early stages;
- Conducting research for children and adults.
Advantages of MRI of cerebral vessels in Magnesia
We conduct a full-fledged study of the entire vascular system of the brain: we look at the arteries, veins, and venous sinuses at once. We do not divide the vascular system of the brain into subtypes, unlike many other centers, since dividing it and looking at it in parts (arteries separately, veins separately) is not logical and is not very informative for a doctor.
The formation and development of the vascular system of the brain in the fetus occurs in one period, and pathological changes can occur in both the arterial and venous systems. As a rule, the pathology of arteries and veins occurs in parallel. A striking example is arteriovenous malformations.
Contraindications to MR angiography
Before magnetic resonance imaging, you should consult your doctor to rule out absolute contraindications. These include:
- the presence of ferromagnetic structures in the body. These can be any structures that cannot be removed independently: prostheses, knitting needles, pins, Ilizarov apparatus, etc.;
- presence of a pacemaker, artificial heart pacemaker, mechanical heart valves;
- ferromagnetic or electronic implants of the middle and inner ear.
Relative contraindications to MR angiography include:
- women do not undergo vascular MRI angiography during the first trimester of pregnancy - this is permissible only if there are serious indications and special instructions from the doctor;
- pathological processes in which a person cannot maintain a still state, neurological diseases;
- fear of confined spaces. If you have claustrophobia or excessive anxiety, you can ask your doctor to prescribe mild sedatives for you before your scheduled test.
Be sure to warn our Center staff about claustrophobia. We suggest being present with one of your relatives or friends, coming early to look at the tomograph and even try to lie down.
- extremely serious condition.
Preparation of MR angiography:
No special preparation is required before angiography.
If you are asthmatic, take your inhaler with you.
SURVEY RESULTS
At Magnesia you will receive a disk with images immediately after undergoing an MRI. The results of the examination (description and conclusion of a specialist) can be given to you within 60-90 minutes after the procedure. If a consultation is necessary, the description can take up to three days. If you wish, you can receive all the necessary information electronically.
Prices and list of vascular MRI services in Kemerovo:
| № | Magnetic resonance studies: | Prices in rubles |
| 2 | Vascular studies: | |
| 2.1 | Brain with angiography of arteries, veins, venous sinuses | 5 400 |
| 2.2 | Angiography of arteries, veins, venous sinuses (done only with/after GM) | 3 000 |
| 2.3 | Cervical spine + neck vessels | 5 800 |
| 2.4 | Neck vessels | 2 700 |
Sign up for an MRI