Why is the research being conducted?
Lipids are complex organic substances. In the human body they perform very important functions:
⦁ are an element of cell membranes; ⦁ serve as a powerful molecular source of energy; ⦁ participate in the synthesis of many hormones, vitamins, biologically active substances; ⦁ transport fat-soluble vitamins and medicinal substances.
Also, the indicator may increase during pregnancy, menopause, with alcohol intoxication, taking diuretics, hormonal drugs, corticosteroids, vitamin D2, and the predominance of cholesterol-rich foods in the diet - eggs, fatty meats.
Low values of the indicator may be the result of liver pathologies, severe acute inflammatory processes, malabsorption syndrome, and a lack of animal products in the diet.
general characteristics
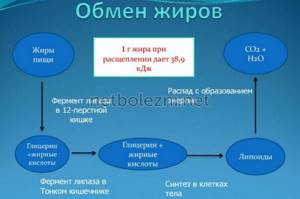
Triglycerides (TG) are simple organic compounds from the group of lipids. These substances enter the body with food and are absorbed in the intestines during the process of breakdown by bile acids. Lipids are also synthesized in the liver from dietary fats and partly from carbohydrates. The release and transformation of substances occurs between meals.
A test to determine triglyceride levels is called a lipid profile.
Simple lipids (VLDL very low density lipoproteins) act as structural cellular material and participate in the processes of cellular nutrition.

These substances have several meanings:
- are the main material that makes up the cell membrane;
- create energy reserves by forming a fat layer;
- participate in cholesterol transport.

TG are contained in the blood in the form of soluble lipoproteins (in complex with proteins), which facilitates their transportation. Circulating in the blood, these compounds are hydrolyzed in cardiac muscle tissue, skeletal muscle fibers and adipose tissue.
Blood pressure is one of the indicators of human health. A condition in which blood pressure is too low is called hypotension or arterial hypotension. Read more in the article: “low blood pressure in women: signs, symptoms and treatment.”
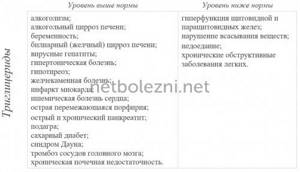
Causes of increased triglycerides
A condition in which women have abnormally high levels of triglycerides in the blood is a type of hyperlipidemia called hypertriglyceridemia. This pathology occurs in the following cases:
- as a consequence of various disorders in the departments responsible for the synthesis and transformation of triglycerides;
- as a result of a genetically inherited tendency to increase triglycerides.
In addition to high TG levels, with hypertriglyceridemia, tests monitor an increase in other types of lipoproteins.
Features of hypertriglyceridemia
A lipidogram involves taking and photometrically examining blood from a vein. As part of the biochemical analysis, the level of TG and other lipids, including total cholesterol (cholesterol), is determined. The blood lipid profile allows you to determine triglycerides in the blood (the norm in women corresponds to the reference values given in the table) and diagnose the presence or absence of pathological changes.
Stroke is one of the most common causes of death in people over 30 years of age. The danger is that it begins suddenly and quickly causes irreversible damage, so it is important to provide the patient with the necessary assistance in a timely manner. Read more in the article: “signs of stroke at a young age.”
| Woman's age, years | TG norm, mmol/l | Total cholesterol | ||
| optimal | acceptable | critical | ||
| 18-25 | 0,5-1,4 | 5,16 | 6,18 | 6,22 |
| 25-35 | 0,5-1,7 | |||
| 35-45 | 0,6-2 | |||
| 45-65 | 0,6-2,6 | |||
| 65 and older | 0,6-2,7 | |||

If there is a high level of triglycerides in the blood, then other lipids will also be elevated. A high TG level in an adult has a double meaning. When conducting diagnostics, it is determined as follows:
- as a risk factor for the development of diseases of the heart, blood vessels and other dependent departments;
- as a diagnostic criterion for a number of cardiovascular and endocrine, hepatobiliary and intestinal pathologies.
This indicator as part of the lipid profile allows you to assess the risks of developing pathological changes, track the dynamics of the patient’s condition and adjust the diet at high concentrations of exogenous lipids.
[media=
https://youtu.be/WAmaBENp8RM
]
The state of lipid metabolism in women with early menopause and hypothyroidism
The prevalence of metabolic syndrome (MS) is reaching epidemic proportions, which requires the integration of various medical specialties for the purpose of timely diagnosis, effective treatment and prevention. Impaired lipid metabolism (dyslipidemia) is one of the main factors in the development of MS. In patients with MS, there is often a combination of “traditional” risk markers for coronary heart disease (CHD) (increased levels of cholesterol (CH), low-density lipoproteins (LDL), decreased levels of high-density lipoproteins (HDL)) with non-traditional ones - increased concentrations of triglycerides ( TG), small modified LDL particles (very low density lipoproteins (VLDL)), low HDL levels. It has now been proven that an increase in the level of TG, VLDL and a decrease in the level of HDL are independent factors of coronary artery disease, and also reflect the effect of lipid-lowering therapy.
Dyslipidemias are classified depending on which specific lipids and lipoproteins levels are outside the normal range. According to Fredrickson's classification (1967), 5 phenotypes of dyslipidemia are distinguished. Type I is characterized by an increase in chylomicrons, TG, cholesterol, for type IIa - an increase in LDL, cholesterol (may be normal), for type IIb - an increase in LDL, VLDL, TG, cholesterol, for type III - VLDL, TG, cholesterol, chylomicrons, for type IV - increased VLDL, TG, cholesterol (may be normal), for type V - increased VLDL, chylomicrons, cholesterol, TG. The risk of developing atherosclerosis increases sharply for coronary and peripheral vessels, starting with type IIa.
But this classification does not separate primary and secondary dyslipidemias and does not take into account the level of HDL and genetic defects that underlie many lipid metabolism disorders. Dyslipidemia can only be characterized by an increase in cholesterol (isolated hypercholesterolemia), triglycerides (isolated hypertriglyceridemia), triglycerides and cholesterol (mixed hyperlipidemia).
Primary dyslipidemias are determined by single or multiple mutations of the corresponding genes, as a result of which there is overproduction or impaired utilization of triglycerides and LDL cholesterol or overproduction and impaired clearance of HDL. Primary dyslipidemias can be diagnosed in patients with clinical symptoms of these disorders, with early onset of atherosclerosis (before 60 years of age), in those with a family history of atherosclerosis, or with elevated serum cholesterol levels > 240 mg/dL (> 6.2 mmol/L).
Secondary dyslipidemias usually occur in the population of developed countries as a result of a sedentary lifestyle and consumption of food containing large amounts of cholesterol and saturated fatty acids. Another cause of secondary dyslipidemia may be the development of diseases such as hypothyroidism, estrogen deficiency, diabetes mellitus, etc.
Up to 45–50 years of age, women have a significantly lower risk of developing atherosclerosis compared to men, which is largely due to the protective properties of estrogens, which maintain lipid concentrations within optimal values. However, with the sharp onset of estrogen deficiency, the factors for the development of metabolic disorders increase [1, 2]. The protective effect of estrogens on lipid metabolism is as follows: the production of large, TG-rich VLDL particles increases, which is accompanied by an increase in the level of total TG in the blood; the LDL content decreases by increasing the number of liver receptors for LDL, which subsequently leads to increased catabolism; Estrogens can inhibit the activity of hepatic triglyceride lipase, which leads to an increase in HDL levels due to a delay in their clearance.
The second feature of a deficiency in ovarian estrogen production is a change in the level of gonadotropin production by the pituitary gland and, in particular, an increase in the level of follicle-stimulating hormone (FSH), luteinizing hormone (LH), and thyroid-stimulating hormone (TSH). The prevalence of overt hypothyroidism in the general population is about 2%, and it is 10 times more common among women [4]. Subclinical hypothyroidism (SH) or minimal thyroid deficiency is a condition in which hormonal testing reveals normal free thyroxine (T4) levels and elevated TSH levels. Subclinical hypothyroidism is more common than manifest hypothyroidism - its prevalence varies from 8% to 10% among women [5]. It is interesting to note that among menopausal women, the prevalence of FH increases in direct proportion to cholesterol levels: from 4% in women with low cholesterol levels to 10% in women with the highest cholesterol levels. In addition, it has been shown that in postmenopausal women, an increase in TSH levels by 1 mU/L is accompanied by an increase in cholesterol levels by 0.09 mmol/L (3.5 mg/dL) [5].
Dyslipidemia, which is observed in hypothyroidism, is characterized by an increase in serum levels of VLDL and LDL, which is caused by a deficiency of thyroid hormones, which leads to a decrease in the content of LDL receptors in the liver and, consequently, to a decrease in hepatic excretion of cholesterol and, subsequently, to an increase in the level of LDL and VLDL, rich in apo-B-lipoproteins [6]. LDL receptor expression is negatively regulated by intracellular cholesterol levels mediated by sterol binding regulatory protein-2 (SSRP-2). With long-term hypothyroidism, the structure of HDL is disrupted and the reverse transport of cholesterol is impaired, which is the main anti-atherogenic process in the human body [7]. Studies evaluating the effects of thyroid hormone replacement therapy on lipoprotein levels in patients with thyroidectomy have not found changes in the apolipoprotein (apo-C3) (HDL)/apo-C3 (LDL) ratio, which provides an indirect measure of lipoprotein lipase activity ( LPL), which indicates that in hypothyroidism the activity of this enzyme is not impaired [7].
HDL has the most pronounced antiatherogenic properties; their level is regulated by another key enzyme—hepatic lipase (LLP) [8]. Lipid exchange between lipoproteins is carried out by cholesterol ester transport protein (CETP), which transfers cholesterol esters from HDL to VLDL, and triglycerides back to HDL. Thyroid hormones stimulate fat utilization, mobilization of triglycerides from adipose tissue and activate PL and CETP [6, 8]. CETP is a plasma protein that, as previously stated, mediates the exchange of cholesteryl esters between lipoproteins and is a key factor in HDL metabolism and reverse cholesterol transport pathways. Consequently, a decrease in CETP activity may lead to disruption of these processes. Hepatic lipase (HL) is a glycoprotein produced by the liver that promotes the remodeling of various lipoproteins. With long-term hypothyroidism, a significant decrease in the activity of CETP and PL, which provide approximately 30% of reverse cholesterol transport, can occur [8]. In addition, a decrease in the activity of CETP and PL in hypothyroidism can lead to impaired conversion of LDL to HDL [9]. As a result, there is an increase in serum levels of VLDL, apo-B, LDL and HDL.
Diagnostics
To assess the state of the hypothalamic-pituitary ovarian function in women with early shutdown of ovarian function, it is necessary to conduct a study of the level of FSH, LH, steroid hormones - estradiol, progesterone, androgens in the blood serum.
Diagnosis of hypothyroidism is very specific and accessible. It involves determining the level of TSH and T4, while the detection of an isolated increase in TSH (4.0–10.0 mIU/l with a norm of 0.4–4.0 mIU/l) indicates subclinical hypothyroidism, and a simultaneous increase in TSH level and a decrease T4 level - about obvious or manifest hypothyroidism. The 2000 American Thyroid Association guidelines recommend screening TSH levels at 5-year intervals in all adults over the age of 35 years. The feasibility of population screening is due to the significant prevalence of various thyroid dysfunctions. In addition, subclinical hypothyroidism may be associated with hypercholesterolemia that is reversible with replacement therapy, especially in cases where the TSH level exceeds 10 mIU/L. Determination of TSH levels is an accurate, widely available, reliable and relatively inexpensive test for diagnosing any type of thyroid dysfunction [3].
Diagnosis of dyslipidemia is made on the basis of determining the indicators of cholesterol, TG, HDL, LDL and LDL (Table 1).
During the day, even healthy people have fluctuations in cholesterol levels by 10%; TG parameters - by 25%. LDL content is calculated using the Friedewald formula: LDL = cholesterol - (HDL + triglycerides/5), based on the fact that LDL is the amount of cholesterol minus the cholesterol contained in VLDL and HDL. The amount of cholesterol in VLDL is equal to triglycerides/5, since the concentration of cholesterol in VLDL is approximately 1/5 of the total amount of lipids (Table 2).
Fasting lipid profiles are measured in individuals over 20 years of age every 5 years. In this case, it is necessary to identify other risk factors for the development of cardiovascular diseases (diabetes mellitus, smoking, arterial hypertension, family history of the development of coronary artery disease in first-degree relatives).
To assess the ratio of atherogenic and antiatherogenic fractions of cholesterol, we used the cholesterol atherogenicity coefficient proposed by A. M. Klimov (1977), calculated by the formula: CAT = (total cholesterol (TC) - HDL cholesterol)/HDL cholesterol.
Treatment
Considering the frequent development of dyslipidemia against the background of a combination of estrogen and thyroid hormone deficiency in women, timely recommended hormone replacement therapy can reduce the risk of mortality from cardiovascular pathology by 9–13%.
The drug Eutirox belongs to the pharmacological group of thyroid hormone drugs, the active substance of which is levothyroxine sodium (L-thyroxine, L-T4). L-T4 therapy for hypothyroidism is rightly considered the “gold standard”. The action of the drug Eutirox is identical to the action of natural thyroxine. The drug is characterized by high bioavailability (more than 80% when taken orally) and good tolerability, with a long half-life in plasma (about 7 days). When taking Eutirox, side effects are practically absent and can only occur in case of overdose. The daily rhythm of thyroid hormone secretion is practically absent (variation from day to day is less than 15%). In this regard, daily administration of the drug Eutirox in the same dose easily models their endogenous production. The drug should be taken in the morning on an empty stomach 30–40 minutes before meals, once a day, at the same time of day and at least 4 hours apart before or after taking other medications or vitamins. Dosages: 25, 50, 75, 100, 125 and 150 mcg. The quality of life of patients with hypothyroidism who are constantly receiving replacement therapy with Eutirox is almost insignificantly different from that for persons without hypothyroidism.
In case of manifest hypothyroidism, replacement therapy with levothyroxine is indicated at an average dose of 1.6–1.8 mcg/kg of the patient’s body weight. The criterion for the adequacy of this therapy is the persistent maintenance of normal TSH levels in the blood.
For subclinical hypothyroidism, it is recommended: repeated hormonal testing after 3–6 months to confirm the persistent nature of the thyroid dysfunction; Levothyroxine replacement therapy is indicated for persistent subclinical hypothyroidism (increased TSH levels in the blood by more than 10 mU/l, as well as in the case of at least two detections of TSH levels between 5–10 mU/l).
The criterion for the adequacy of replacement therapy for subclinical hypothyroidism is the persistent maintenance of normal TSH levels in the blood.
To treat ovarian hypofunction, in the absence of contraindications, hormone replacement therapy (HRT) (Femoston) is prescribed. Femoston is a combined two-phase drug for hormone replacement therapy, containing micronized 17-beta-estradiol (1 mg) as an estrogenic component and dydrogesterone (10 mg) as a gestagenic component. Both components are chemically and biologically identical to the endogenous female sex hormones produced in the ovaries (estradiol and progesterone).
Estradiol replenishes the deficiency of estrogen in the female body after menopause and provides effective relief of psycho-emotional and vegetative menopausal symptoms, such as hot flashes, increased sweating, sleep disturbances, increased nervous excitability, dizziness, headache, involution of the skin and mucous membranes, especially the genitourinary system (dryness) and irritation of the vaginal mucosa, pain during sexual intercourse).
Taking Femoston leads to a change in the lipid profile towards a decrease in the level of total cholesterol and LDL and an increase in HDL. Dydrogesterone is a gestagen, effective when taken orally, which completely ensures the onset of the secretion phase in the endometrium, thereby reducing the risk of developing endometrial hyperplasia and (or) carcinogenesis (increased with the use of estrogens). Dydrogesterone does not have estrogenic, androgenic, anabolic or glucocorticoid activity.
After taking the drug orally, micronized estradiol is easily absorbed and subsequently metabolized in the liver to form estrone and estrone sulfate. Estrone sulfate undergoes intrahepatic metabolism. Glucuronides of estrone and estradiol are excreted primarily in the urine.
In the body, dydrogesterone is quickly absorbed from the gastrointestinal tract and completely metabolized. The main metabolite of dydrogesterone is 20-dihydrodydrogesterone, present in urine mainly as a glucuronic acid conjugate. Complete elimination of dydrogesterone occurs after 72 hours.
Indications for prescribing Femoston are: hormone replacement therapy for disorders caused by natural menopause or menopause resulting from surgical intervention; prevention of osteoporosis in postmenopause.
To date, the question of the effect of sex steroid hormone therapy on thyroid status remains insufficiently studied; the data available in the literature on this issue are somewhat contradictory. The only thing that has been reliably established is the impossibility of a direct influence of estrogens on the hormone-producing function of the thyroid gland due to the absence of receptors for estrogens and progesterone in its tissue. Fluctuations in thyroid hormone levels are adaptive in nature during the period of adaptation to HRT. This period in patients with hypothyroidism takes about 6 months, while in women without thyroid pathology, according to the literature, it lasts for 3 months, which may be due to a decrease in metabolism in the liver due to a lack of thyroid hormones. An increase in T4 levels during HRT in women with primary hypothyroidism in menopause can be explained by an increase in the sensitivity of thyrotrophs to TSH estrogens. In this situation, eliminating estrogen deficiency can increase the functional activity of the thyroid gland in the absence of profound irreversible changes in its tissue (Table 3).
At the District Clinical Perinatal Center in Surgut, we examined 45 women with early menopause. The average age of the patients was 32.7 ± 2.3 years. The average duration of the disease was 6.8 ± 1.6 years. The reason for contact was the absence of menstruation, rapid weight gain (on average 10 ± 2.1 kg/year) in 77.8% of patients since the cessation of menstruation. When analyzing the body mass index of women in the clinical group, it was revealed that only 22.2% of patients had normal body weight, 44.4% had a body mass index within the range of overweight, 17.8% had mild obesity, 11 .1% have moderate obesity and 4.4% have extreme obesity.
With an increase in the level of FSH (average value 32.4 ± 8.5 U/ml) and LH (15.8 ± 3.1 U/ml), a decrease in the level of estradiol and progesterone in the blood plasma of patients was observed. The higher the level of FSH in the blood plasma, the more pronounced were the echographic signs of ovarian hypofunction, such as a decrease in ovarian volume (average value 1.25 ± 0.23 cm3), number of follicles (average number - 3.4 ± 1.4 ) and an increase in the resistance index in the ovarian artery (average RI = 0.78). When assessing thyroid function, the average TSH value was 12.3 ± 0.45 IU/l, a decrease in T4 levels in 64.4% of patients. According to ultrasound data, both during combination therapy (simultaneous administration of the drugs Eutirox and Femoston) and during monotherapy with levothyroxine, the volume of the thyroid gland decreased by 8% and amounted to 20.9 ± 1.3 cm3.
We studied and compared the results of lipid metabolism in women. During the initial assessment of the parameters of the blood lipid spectrum, various variants of its disturbance were identified in 93.3% of women with hypothyroidism and early menopause. In hypothyroidism, type IIa dyslipidemia was more common (55.5%), and type IIb, accompanied by an increase in all atherogenic fractions of the lipid spectrum, was detected in 26.6% of cases, while in the euthyroid state only 13.3% had this type. female patients. A detailed study of the concentration of various classes of lipoproteins depending on the functional state of the thyroid gland found that women with uncompensated hypothyroidism have a significantly higher level of cholesterol by 30.3% (p < 0.05), LDL by 18.7% (p < 0 .05), TG by 15.6% (p < 0.05) and atherogenicity coefficient by 58.2% (p < 0.05).
Despite lower concentrations of atherogenic lipid fractions in women without thyroid pathology, these patients had an increase in atherogenic potential, indicating an inversely proportional relationship between the atherogenicity coefficient and the concentration of the antiatherogenic HDL fraction. Thus, we have identified a high incidence of thyroid pathology, in particular hypothyroidism, in women with estrogen deficiency. Both pathological conditions lead to the development of dyslipidemia as one of the manifestations of MS. Complex HRT (Femoston and Eutirox) has a positive effect on blood lipid metabolism, reducing the atherogenicity coefficient by 17.5% (p < 0.05).
Literature:
- Azizova D. Sh. State of lipid metabolism in women with postovariectomy syndrome in conditions of chronic iodine deficiency // Pediatrics. Specialist. release. 2003. pp. 183–189.
- Serebrennikova K. G., Chumakova N. V., Konev M. V. The effect of hormone replacement therapy on some metabolic processes in women with surgical menopause. Materials of the First Russian Congress on Menopause, Moscow, September 10–12, 2001. Menopause. 2001; 3:67.
- Fadeev V.V. Modern concepts of diagnosis and treatment of hypothyroidism in adults // Probl. Endocrinol. 2004. No. 2. P. 47–53.
- Vanderpump MP, Tunbridge WM Epidemiology and prevention of clinical and subclinical hypothyroidism // Thyroid. 2002. Vol. 12. P. 839–847.
- Bindels AJ, Westendorp RG, Frolich M. et al. The prevalence of subclinical hypothyroidism at different total plasma cholesterol levels in middle aged men and women: a need for case finding // Clin Endocrinol. 1999. Vol. 50. P. 217–220.
- Shin DJ, Osborne TF Thyroid hormone regulation and cholesterol metabolism are connected through Sterol Regulatory Element-Binding Protein (SREBP-2) // J Biol Chem. 2003. Vol. 278. P. 34114–34118.
- Dredecjus M., Masson D., Gautier T. et al. Low cholesteryl ester transfer protein (CETP) concentration, normal CETP activity in serum from patients with shortterm hypothyroidism. Lack of relationship to lipoprotein abnormalities // Clin Endocrinol. 2003. Vol. 58. P. 581–588.
- Franco M., Castro G., Romero L. et al. Decreased activity of lecithin: acyltransferase and hepatic lipase in chronic hypothyroid rats: implications for reverse cholesterol transport // Mol Cell Biochem. 2003. Vol. 246. P. 51–56.
- Zambon A., Bertocco S., Vitturi N. et al. Relevance of hepatic lipase to the metabolism of triacylglycerol rich lipoproteins // Biochem Soc Trans. 2003. Vol. 31. P. 1070–1074.
L. D. Belotserkovtseva , Doctor of Medical Sciences, Professor L. V. Kovalenko , Doctor of Medical Sciences, Professor E. V. Korneeva, Candidate of Medical Sciences, Associate Professor
State Educational Institution of Higher Professional Education, Surgut State University of Khanty-Mansi Autonomous Okrug-Yugra, Surgut
Contact information for authors for correspondence
Provoking diseases
In biochemical analysis, elevated triglycerides are a sign of the development of a number of diseases. The following causes of hypertriglyceridemia are distinguished:
- obesity;
- diseases of the cardiovascular system;
- liver and gallbladder diseases;
- pathology of the pancreas;
- intestinal diseases;
- diabetes.

Such conditions are associated with impaired absorption of TG, their remodulation, or with excessive consumption of fatty and carbohydrate foods.
Eating disorders
The main reason for the high concentration of simple fats in the blood is poor nutrition. Women, due to hormonal characteristics, are more prone to accumulating excess weight.
Violation of the diet (with excessive consumption of sweet and fatty foods) contributes to the rapid conversion of triglycerides into fat, since the body is not able to convert all incoming fats into energy. With obesity, undigested fats enter the bloodstream in large quantities, causing cardiovascular and other diseases.
Cardiovascular pathologies
Since the transport and hydrolysis of lipoproteins occurs in the bloodstream and muscle tissue, this affects the condition of the blood vessels. Excess circulating lipids adhere to the inner and outer walls of arterioles, turning into atherosclerotic plaques. Atherogenic factors lead to obstruction of blood flow and the risk of developing coronary heart disease, ischemia and myocardial infarction.

Pathologies of the hepatobiliary tract
One of the triglyceride fractions is resynthesized in the liver tissue and then enters the bloodstream again. There are several diseases that make it difficult for the female body to reabsorb endogenous TG:
- steatosis;
- fibrosis;
- hepatitis A, B, C, D;
- cirrhosis of the liver.

These processes are accompanied by inflammation and changes in structural tissues, causing compression of the bile ducts and blood vessels. As a result of degradation of the parenchyma, an intensive flow of lipoproteins directly into the bloodstream is observed.
Intestinal pathologies
Absorption of triglycerides entering the bloodstream occurs directly in the intestine. Inflammatory processes localized in this part of the digestive tract make it difficult to directly remove excess TG (by separating bowel movements). Excess lipids are absorbed into the bloodstream, so their level in the biochemical analysis is increased.

Inflammation of the pancreas
Inflammatory processes that develop in the pancreas complicate the secretion of digestive enzymes and are a provoking factor for diabetes mellitus.
The interrelated processes that occur during the development of pancreatitis make it difficult to properly absorb exogenous triglycerides.
In acute inflammation, a rapid increase in laboratory parameters is observed, which makes it possible to differentiate the pathology from other abdominal pain.

Reasons for high rates
If you have elevated triglyceride levels, it is due to the following factors:
- High body weight.
- Diabetes.
- Kidney disorders.
- Hereditary lipid imbalance.
- Binge eating.
- Alcohol abuse.
- Atherosclerosis.
- Hypothyroidism.
There may be other reasons:
- Lack of daily routine, unhealthy diet.
- Uncontrolled use of certain medications, such as: corticosteroids, oral contraceptives, beta-blockers.
Elevated levels of blood lipids may indicate the presence of the above pathologies, and the patient will learn about this only after examination. In this case, it is necessary to follow a special diet that helps reduce cholesterol. Significantly increases the risk of heart and vascular diseases, hepatitis in various forms, and liver cirrhosis.
Reasons for the increased rate in women
In adult women, deviations from the norm are observed more often than in men, and the causes of increased triglycerides are usually:
- Taking oral contraceptives containing estrogen.
- Gestational age.
- Polycystic ovary syndrome.
- Menopause period.
- Disruptions at the hormonal level.
- Infertility.
During pregnancy, lipid levels are usually higher than normal, often accompanied by an increase in cholesterol, and this is normal. An increase in this indicator is very concerning, so pregnant women should limit their consumption of foods containing TG to a minimum.
More often, deviations from the norm in this situation arise due to hormonal disorders, less often due to an unfavorable course of pregnancy or abnormalities in the development of the fetus.
With significant overeating disorders during pregnancy, the blood becomes thicker, and the fetus becomes deficient in oxygen and nutrients. In such cases, the doctor selects a suitable and gentle treatment.
Reasons for high values in men
The norm for an adult man is slightly higher than for the fair sex. Its excess is most often caused by the abuse of alcoholic beverages, tobacco products and often manifests itself against the background of stressful situations and overeating.
In children
In a child, excessive frequency is due to the following factors:
- Overweight.
- Poor nutrition.
- Down syndrome.
- Genetic predisposition.
In such situations, the attention and patience of parents is required, since the child must get used to healthy food and exclude all kinds of fast food and chips from the diet.
It is also necessary to give children fish oil. In addition, it is necessary to consult a doctor and undergo a thorough examination.
Risk factors
Several aggravating factors influence the increase in triglyceride levels in the female body. The following parameters are distinguished:
- pregnancy;
- medications (oral contraceptives, cholesterol-lowering drugs, diuretics, glucocorticosteroids, hormonal agents);
- menopause;
- smoking;
- excessive consumption of alcoholic beverages;
- consuming large amounts of saturated (animal) fat.

A sedentary lifestyle also has a negative effect on TG metabolism. Low physical activity significantly reduces the conversion of fat into energy and leads to high triglyceride concentrations.
In addition to endogenous factors, hyperlipidemia can be a consequence of causes due to hereditary factors.
Converting fats into energy is difficult in the following cases:
- low metabolic rate due to genetic factors;
- hereditary tendency to inflammatory and atherogenic processes.

Hypertriglyceridemia also develops with hereditary defects in the structure of the gastrointestinal tract, hepatobiliary tract and cardiac structure.
How to reduce high TG levels
A prerequisite for normalizing triglycerol levels is a special diet:
- Fast carbohydrates are replaced with complex ones: when consuming polysaccharides and limiting glucose, the risk of such a problem is minimal.
- The amount of saturated fat is minimized, giving preference to seafood that contains polyunsaturated fatty acids.
- It is better to replace industrial mayonnaise and other products containing trans fats (spread, margarine) with olive oil.
- Metabolic processes can be activated with adequate energy loss. Instead of alcohol and nicotine, physical activity will give you energy and good mood.
- It is important to promptly treat all inflammations and infectious diseases.
At the initial stage, such measures will be sufficient; if the problem has gone beyond prevention, the doctor will prescribe a lipid profile, analyze the functioning of the heart and recommend appropriate drug treatment.
Features of laboratory analysis
To obtain objective data, several conditions must be met when performing a lipid profile. The preparatory stage contains the following recommendations:
- 24 hours before the test, drinking alcohol is prohibited;
- the analysis is carried out on an empty stomach;
- at least 24 hours of dietary nutrition, low in fat.

Failure to comply with these requirements may result in distorted results. If there is a hereditary tendency to increase cholesterol, it is recommended to carry out the analysis up to 2 times a year.
Triglyceride test
Triglycerides in the blood reflect the body's energy balance. Medical specialists recommend regularly diagnosing TG values - for people over 20 years of age, once every five years is optimal.
There are a number of medical indications for analysis, namely:
- high blood pressure (blood pressure),
- a history of diabetes mellitus,
- long-term bad habits - smoking, alcohol abuse, excess body weight, physical inactivity (inactive lifestyle),
- older age.
(1 rating, average 4 out of 5)