More about the service
Prenatal screening is a complex procedure aimed at identifying pathologies of fetal development in the 1st and 2nd trimesters of pregnancy.
Thanks to screening, a specialist can assess the health status of an unborn baby and determine the possible risk of developing genetic diseases. The procedure is not the final verdict on whether the baby will be born with an abnormality or disease. It provides information about the presence of the risk itself. After studying the results of prenatal screening, the geneticist may prescribe additional clarifying studies. Only after this are final conclusions made.
Invasive methods.
The most reliable way to make a diagnosis is karyotyping - a study that looks at the number of chromosomes and their quality. In the first trimester, it is possible to use two invasive diagnostic methods - amniocentesis and chorionic villus biopsy.
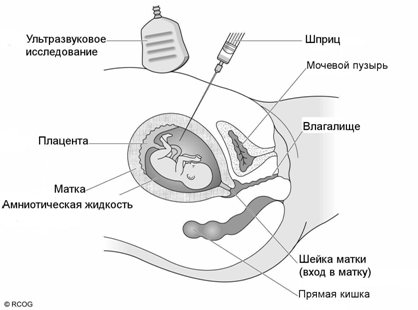
- Amniocentesis is the removal of a small amount of amniotic fluid (about 25 ml), which contains fetal cells. As a rule, this is a short procedure, which in terms of pain can be compared to a regular blood draw. The manipulation involves the introduction of a thin game, and in case of access through the vagina, a catheter into the uterine cavity through the amniotic membrane under the control of an ultrasound sensor. This invasive procedure carries minimal but risks associated with premature birth. When performing amniocentesis, the risk of miscarriage is 01%-0.25%. After the study, it is recommended to rest, not exercise for 48 hours and to abstain from sexual intercourse for 72 hours.
- Chorionic villus biopsy. To begin with, it’s worth saying what kind of structure this is. The chorion is one of the membranes around the baby. Both the membranes and the fruit developed initially from one cell. Their genetic composition is identical, therefore, by taking a small number of chorion cells, we can evaluate the child’s karyotype. The biopsy is performed via transabdominal or vaginal access. Under the control of an ultrasound sensor, a needle is inserted, which captures part of the villi cells. The risk of preterm birth is higher than with amniocentesis, but is less than 1%. Next, the material is sent to the laboratory for karyotyping.

There is another test for identifying chromosomal pathologies, which is not as common in Russia as invasive screening. NIPT (NIPT or cfDNA) is a non-invasive test to identify fetal cells circulating in the mother's body, which are subsequently also karyotyped. Today, this test is not included in the compulsory medical insurance program, but is produced by many private laboratories. Manufacturers of the test claim 99% accuracy for Down and Edwards syndrome, and 72-92% for diagnosing Patau syndrome.
However, there are also limitations:
- number of fruits more than 2;
- if there are signs of a frozen singleton pregnancy;
- the pregnant woman underwent organ and tissue transplantation, including bone marrow, before pregnancy;
- if the mother has cancer.
The variability of the screening panels is another feature of this test. If during an invasive study we look at the complete karyotype of the fetus, then with NIPT we look for specific mutations.
Prenatal screening 1st trimester
According to the rules, prenatal screening of the 1st trimester is done at 10-13 weeks. By the 10th week, the embryo becomes a fetus, around which the placenta forms. The baby's internal organs are already congested, and you can hear his heartbeat. Prenatal screening of the 1st trimester consists of 2 procedures: study of blood parameters and ultrasound of the fetus.
Prenatal biochemical screening: blood test
This is the most important and very informative procedure that every pregnant woman needs to undergo.
- Biochemical analysis of venous blood. Genetic studies are carried out using markers and DNA sequences. Screening for trisomy 13, 18 and 21 reveals the incorrect combination of genes obtained when the germ cell divides and turns the fertilized egg into an embryo. A sick child inherits not two chromosomes, but three, which interferes with his physical and mental development in the future. With an extra 13th chromosome, Patau syndrome develops; with the 18th and 21st chromosomes, Edwards and Down syndromes develop. If trisomy screening confirms the presence of anomalies, the woman undergoes a chorionic villus biopsy - a study of the villi covering the fetal membrane. This study provides an accurate answer to the question of whether the child has a genetic pathology.
- Determination of pregnancy hormone levels. When the fetus implants in the uterus, the level of the hormone human chronic hydrotropin increases sharply. If the mother does not have diabetes mellitus or multiple pregnancy, a significant increase in hCG indicates the presence of pathologies in the fetus.
- Determination of the level of placental lactogen. This hormone, produced by the placenta, protects the fetus: it lowers glucose levels, produces amino acids, and also suppresses the immune system if the mother’s body does not perceive the unborn baby as “native” - i.e. The woman's body rejects the fetus. A decrease or increase in the level of placental lactogen indicates an abnormality in the development of pregnancy.
- Determination of free estriol level. Its concentration is an accurate marker of the presence of pathologies in a baby, for example, if the parents are close relatives. A decrease in estriol indicates hydrocephalus, anencephaly (absence of the brain) in a child, Down, Patau and Edwards syndromes, and other disorders
- Determination of PAPP-A protein level. This plasma protein is produced in large quantities only during pregnancy. The level of PAPP-A protein is used to judge possible spontaneous abortion, chromosomal abnormalities in the fetus, etc.
- Inhibin A level. The indicator increases 2 times if the baby has Down syndrome. This is also a placental hormone (hydroprotein), which is used to judge the development of pregnancy.
All tests are performed on an empty stomach. Before the procedure, a woman needs to get enough sleep, avoid stress and be positive.
Ultrasound diagnosis of the fetus during prenatal screening in the 1st trimester
Ultrasound in the early stages is performed using two-dimensional or three-dimensional echography. Despite the fact that the size of the fetus is still only a few centimeters, ultrasound diagnostics is very informative. For example, only during this period can an important study be performed - ultrasound of the fetal collar area. Excess lymph fluid in the collar area indicates the possible development of anomalies - this is a signal that the mother needs to be examined more carefully. After the 13th week of pregnancy, the lymphatic system is fully formed, and lymph enters the blood, spreading throughout the body.
Ultrasound shows the number of embryos, the exact duration of pregnancy, the size of the fetus, its placement in the uterus, the approximate outline of the skeleton, reveals the correct position of organs, the symmetry of brain development, the proportionality of bone development. The doctor also examines the structure of the nasal bone - a sign that excludes Down syndrome.
Diagnostic window in the 3rd trimester of pregnancy
The third screening period (32 weeks 0 days - 34 weeks 6 days of pregnancy) has two main objectives: exclusion of congenital malformations with late manifestation and assessment of the condition of the fetus. Issuing a referral for a third ultrasound along with 30 weeks of maternity leave. 0 days of pregnancy potentiates untimely early referral of pregnant women for the third screening ultrasound before 32 weeks 0 days, which in turn may require a repeat planned ultrasound within the “due time”. A later appearance (after 34 weeks) reduces the quality of the image obtained by ultrasound due to a change in the relationship between the amount of amniotic fluid and the volume of the fetal body towards the latter. Therefore, the “ happy days” of the third trimester can be considered the period 32 weeks 0 days - 33 weeks 3 days of pregnancy .
An unscheduled ultrasound at any stage is required, as a rule, only in case of complicated pregnancy, therefore it is prescribed only according to indications and is performed regardless of the gestational age.
Notes: 1 — Order of the Health Committee of the Government of St. Petersburg dated February 1, 2012 N 39-r “On measures to reduce hereditary and congenital diseases in children in St. Petersburg.” 2- Article 56 “Artificial termination of pregnancy”. Federal Law of the Russian Federation of November 21, 2011 N 323-FZ “On the fundamentals of protecting the health of citizens in the Russian Federation”, entered into force: November 22, 2011, published on November 23, 2011 in “RG” - Federal issue No. 5639
Prenatal screening 2nd trimester
2nd trimester screening begins at 16-18 weeks of pregnancy. At this time, you can perform a 4D ultrasound. During this period, the fetus reaches 20 cm, you can examine the child’s face, determine the proportionality of the development of the limbs, the correct formation of organs. 4D ultrasound also shows how mobile the fetus is and determines the sex.
In cases where analyzes of previous results have shown the presence of abnormalities, the expectant mother is recommended to undergo repeated prenatal biochemical screening. It is also mandatory to undergo 2nd trimester screening if:
- the expectant mother or father is over 35 years old - at this age the risk of genetic abnormalities and mutations transmitted by germ cells increases;
- the woman has previously had miscarriages or frozen pregnancies;
- it seems that the parents had children with genetic disorders;
- one of the relatives had children with Down syndrome.
Biochemical analysis includes measuring the level of hormones in the blood: hCG, AFP (alpha-fetoprotein), free estriol. Screening analyzes for the 1st and 2nd trimesters are similar, and if the first results did not reveal any abnormalities, then the 2nd trimester screening is also very likely to go well.
In what cases is the first screening mandatory?
These studies should be carried out on every pregnant woman at 11-13 weeks. Unfortunately, no one is immune from possible pathologies. There is a high risk group:
- parents of the baby who are closely related;
- women who have previously had miscarriages or premature births (more than two);
- women who have had cases of missed abortion or stillbirth;
- women who have had viral or bacterial infections during pregnancy.
Remember that these examinations are important primarily for the health of your baby!
Prenatal screening results
It is important to understand that the screening results are influenced by factors such as the use of drugs and medicines in the period preceding the tests, past stress, increased uterine tone, the weight of the mother and fetus, and the woman’s well-being, so the interpretation of the results is carried out exclusively by a geneticist.
The final results of prenatal screenings are assessed using a special computer program. Women with an indicator of 1:300 are at risk - this is a high risk of having a baby with an anomaly. In 2% of cases, the tests are false positive, so before making a conclusion, the geneticist will conduct a genetic examination using invasive diagnostic methods, when biomaterial is taken from the fetus itself. This procedure will finally answer the question of whether the child has pathologies.
What to do if a fetal malformation is detected?
In the event that a developmental defect is detected in the fetus, further pregnancy management tactics are chosen by the perinatal council of doctors, which consists of an obstetrician-gynecologist, a neonatologist and a pediatric surgeon. There may be several solutions: the defect is considered minor and does not affect the prognosis of life; surgical correction is possible immediately after the birth of the child or intrauterine surgical correction (in extremely rare cases).
Recommendations for termination of pregnancy are made in the event of an unfavorable prognosis for the life and health of the child after birth. The attending physician provides complete information to the pregnant woman about the detected developmental anomaly, the prognosis of the life of the newborn, treatment methods, associated health risks for the mother and child, possible options for medical intervention, their consequences and results. However, the final decision to continue or terminate the pregnancy is made only by the woman!







