Laparoscopic cholecystectomy (also called endoscopic cholecystectomy or gallbladder laparoscopy) is surgery to remove the gallbladder and is the most effective treatment for gallstones. The operation is low-traumatic and is performed endoscopically, i.e. without large cuts. According to statistics, cholecystectomy is the most common laparoscopic operation in the world. The technology of surgical treatment has been developed and gives good results.
Cholecystectomy was first performed in Germany in 1882 by Karl Langebuch. The first patient was discharged after 7 weeks. The first laparoscopic cholecystectomies in the world began to be performed in 1985-1987.
Depending on the category of complexity from 90,000 - 130,000 rubles.
Included in the price:
the operation itself, anesthesia, dressings, medications, food and hospital stay
25-30 minutes
(duration of procedure)
3 days in hospital
Indications
- Presence of stones or polyps in the gallbladder (regardless of clinical manifestations)
Contraindications
- Only severe concomitant diseases can be a contraindication to surgery. In this case, surgical treatment is carried out only for health reasons.
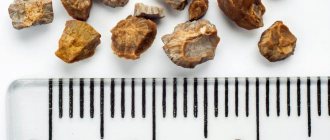
What is gallstone disease?
Gallstone disease (GSD) or cholelithiasis are stones formed in the bile ducts (gallbladder and ducts). The reasons for the formation of stones have not been fully studied, however, there are factors that influence their occurrence: gender, age, pregnancy, dietary habits, various diseases of the hepato-biliary zone and other factors leading to disruption of the stability of the colloidal state of bile and the formation of stones in the gall bladder.
The main symptoms of cholelithiasis are: pain in the right hypochondrium of a cutting or stabbing nature with irradiation to the lower back, right shoulder blade, nausea, vomiting. However, a wide variety of symptoms of the disease are possible: from chest pain to jaundice.
It happens that gallstones do not cause painful symptoms at all and are an incidental finding during an ultrasound or computed tomography. In most such cases, the therapist, gastroenterologist, and often the patient himself decide to postpone the visit to the surgeon until severe symptoms of the disease appear.
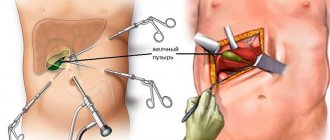
Progress of the operation
Laparotomy cholecystectomy is performed under general anesthesia and lasts approximately 40 minutes. The steps of the procedure are as follows:
- Carbon dioxide is injected into the abdominal cavity.
- Tubes with valves are inserted so that instruments can be inserted without releasing gas, and a tube with a video camera - a laparoscope. The monitors reflect the progress of the operation with multiple magnification.
- Trocars are installed.
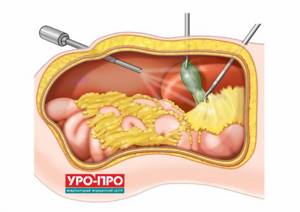
- The gallbladder is held with special instruments and the duct and artery are clamped with clips.
- The gallbladder is separated and removed.
- The abdominal cavity is drained.
Why is surgical treatment of cholelithiasis necessary?
- By delaying a planned operation, you can only wait for an exacerbation or complications of the disease, and performing an emergency operation significantly increases the operational and postoperative risks. Karl Langebuch said that it is necessary to remove the gallbladder “not because there are stones in it, but because it forms them.”
- Today, laparoscopic cholecystectomy (endoscopic removal of the gallbladder along with stones) is the most effective method of treating cholelithiasis.
- Removing the gallbladder eliminates the problem of cholecystitis, practically does not change the quality of life after surgery, and allows you to insure you against many possible and sometimes dangerous complications of cholelithiasis.
Bibliography prof. Konstantin Viktorovich Puchkov in single-portal surgery
- Puchkov K.V., Andreeva Yu.E. Transvaginal cholecystectomy: technical aspects and advantages of the method // Endoscopic surgery. – 2009.-T.15, No. 1. – P.198-199.
- Puchkov K., Andreeva Y., Melnikov. NOTES – technologies in pelvic surgery // Abstracts book of the 13th World Congress on controversies in obstetrics gynecology & infertility, November 4-7, 2010, Berlin, Germany. – P.17-18.
- Forgione A., Puchkov KV, Andreeva YE, Kislov V., Sosnin N., Pugliese R. Transvaginal endoscopic cholecystectomy: the first 100 cases. Operative and long-term results from an international multicenter study group // Abstracts book of the 18th EAES Congress 2010, 16-19 June, 2010, Geneva, Switzerland. – P.94.
- Puchkov K., Andreeva Y., Melnikov. SILS (Single Incision Laparoscopic Surgery) laparoscopic hysterectomy // Abstracts book of the 13th World Congress on controversies in obstetrics gynecology & infertility, November 4-7, 2010, Berlin, Germany. – P.17.
- Puchkov K., Andreeva Y., Melnikov. NOTES – technologies in pelvic surgery // Abstracts book of the 13th World Congress on controversies in obstetrics gynecology & infertility, November 4-7, 2010, Berlin, Germany. – P.17-18.
- Puchkov K.V., Andreeva Yu.E., Melnikov A.L. Optimization of surgical minimally invasive access in the treatment of cholelithiasis // Almanac of the Institute of Surgery named after. A.V. Vishnevsky. T.6, No. 1 (1) - 2011. “Materials of the XIV Congress of the Society of Endoscopic Surgeons of Russia.” – Moscow, 2011. – P. 214-215.
- Puchkov K.V., Andreeva Yu.E., Melnikov A.L.. Laparoscopic hysterectomy through the SILS port (COVIDIEN) // Bulletin of St. Petersburg University. Series 11. Medicine. - 2010. - All-Russian Forum “Pirogov Surgical Week” (appendix) - pp. 824-825.
- Puchkov K.V., Andreeva Yu.E., Melnikov A.L. Single port surgery: indications, advantages, limitations // Almanac of the Institute of Surgery named after. A.V. Vishnevsky. T.6, No. 1 (1) - 2011. “Materials of the XIV Congress of the Society of Endoscopic Surgeons of Russia.” – Moscow, 2011. – P. 213-214.
- Puchkov K.V., Andreeva Yu.E. Experience in performing operations using a single access in surgery and gynecology // Scientific-practical. conf. with international participation in “Technology of single laparoscopic access in abdominal surgery.” – M.: Publishing House “MEDPRACTIKA-M”, 2011.- P.24-26.
- Puchkov K.V., Khubezov D.A., Ogoreltsev A.Yu., Lukanin R.V., Semionkin E.I. Single-port laparoscopic (SILS) colproctectomy with ileoanal reservoir anastomosis // Coloproctology - 2011. - No. 2 (36). - P. 9-12.
- Puchkov K.V., Khubezov D.A., Ogoreltsev A.Yu., Lukanin R.V., Andreeva Yu.E. Single-port laparoscopic (SILS) colproctectomy with ileoanal pouch anastomosis // Fifth International Conference. Russian school of colorectal surgery. "Multidisciplinary approach in the treatment of rectal cancer." Conference materials. - Moscow, June 23-24, 2011 - P. 48.
- Puchkov K.V., Khubezov D.A., Ogoreltsev A.Yu., Lukanin R.V. Experience of laparoscopic SILS colproctectomy with ileoanal reservoir anastomosis and preventive ileostomy // Materials of the 3rd All-Russian Congress of Coloproctologists, October 12-14. 2011, Belgorod, Coloproctology - 2011. - No. 3 (37). - P. 115.
- Puchkov K.V., Khubezov D.A., Ogoreltsev A.Yu., Lukanin R.V., Andreeva Yu.E. Single-port laparoscopic (SILS) coloproctectomy with ileoanal pouch anastomosis // Scientific-practical. conf. with international participation in “Technology of single laparoscopic access in abdominal surgery.” – M.: Publishing House “MEDPRACTIKA-M”, 2011.- P.26-28.
- Puchkov K.V., Andreeva Yu.E., Dobychina A.V. Experience in performing operations using single access in gynecology // Journal. obstetrics and women's diseases.-2011.-T. 60. (special issue). – P.72-73.
- Puchkov K., Andreeva Y., Serebryanskiy O., Dobychina A. Our experience of performing laparoscopic hysterectomy by using SILS-port // Gynecol Surg, 2011, 8 (Suppl). – P.155.
- Puchkov KV, Andreeva YE, Khubezov DA, Puchkov DK The idea is to optimize the choice of a method of operation for the treatment of cholelithiasis (laparoscopy, minilaparoscopy, SILS port, NOTES) // Abstracts book of the 20th EAES Congress 2012 , 20-23 July, 2012, Brussels, Belgium. – P.126.
- Puchkov KV, Andreeva YE, Puchkov DK SILS technology in surgery and gynecology // Abstracts book of the 20th EAES Congress 2012, 20-23 July, 2012, Brussels, Belgium. – P.161.
- Puchkov K.V., Puchkov D.K. Transluminal (NOTES) minilaparoscopic-assisted cholecystectomy - a new “word” in the treatment of cholelithiasis // Endoscopic surgery. – 2013. - Issue No. 2., No. 1. – P.185-186.
- Puchkov DK, Puchkov KV Evaluating the effectiveness of different endoscopes while performing minilaparoscopy-assisted natural orifice (MANOS) cholecystectomy // Abstract book of the 21st International Congress of the EAES. – Vienna, 2013.
- Puchkov KV, Puchkov DK Simultaneous laparoscopic right hemicolectomy with intraperitoneal performing of anastomosis, hysterectomy with transvaginal extraction of colon // Abstract book of the 21th International Congress of the EAES. – Vienna, 2013.
- Puchkov KV, Dobychina A., Korennay V., Puchkov DK Simultanious single and multi-port laparoscopic surgery in gynecology // Abstract book of the 21st International Congress of the EAES. – Vienna, 2013.
- Puchkov KV, Puchkov DK Minilaparoscopy-assisted natural orifice (MANOS) cholecystectomy – a new “word” in the treatment of gallstone disease // Abstract book of the 21th International Congress of the EAES. – Vienna, 2013.
- Puchkov K.V., Puchkov D.K., Khubezov D.A. Transluminal (NOTES) minilaparoscopically assisted, single-puncture and traditional laparoscopic cholecystectomy - what to choose? Evaluation of the results of treatment of patients with uncomplicated cholelithiasis and gallbladder polyposis // Endoscopic surgery. – 2013. – No. 6. – P.16 – 22.
- Puchkov K.V., Puchkov D.K., Khubezov D.A. Laparoscopic cholecystectomy using a single laparoscopic approach technique. A new method for the treatment of chronic cholelithiasis and gallbladder polyposis // Kuban Medical Bulletin. – 2013. – No. 5. – P. 155 – 160.
- Puchkov K.V., Puchkov D.K. Comparative assessment of the use of minimally invasive laparoscopic techniques in the treatment of gallbladder diseases // Endoscopic surgery. – 2014. – T20. - No. 1. – P. 326 – 327.
- Puchkov K.V., Puchkov D.K. Results of the use of minimally invasive laparoscopic techniques in the treatment of cholelithiasis and gallbladder polyposis // Materials of the International Scientific and Practical Conference “Endovideosurgery in a Multidisciplinary Hospital”, St. Petersburg: Publishing House “Man and His Health”, 2014 – P. – 98 – 100. ISBN 978-5-9905495-4-8.
- K. V. Puchkov, D. K. Puchkov, D. A. Khubezov. Transluminal hybrid mini-laparoscopically assisted cholecystectomy is a new step in the evolution of surgery without scars // Journal named after Academician B.V. Petrovsky. – 2014. – No. 3. – P. 48 – 54.
- Puchkov K.V., Puchkov D.K. Results of the use of minimally invasive laparoscopic techniques in the treatment of gallbladder diseases // Almanac of the Institute of Surgery named after. A.V. Vishnevsky. T.10, No. 1 - 2015. “Materials of the XVIII Congress of the Society of Endoscopic Surgeons of Russia.” – Moscow, 2015. – P. 339-340.
- Puchkov K.V., Puchkov D.K. Comparative assessment of the use of modern laparoscopic techniques in the treatment of benign diseases of the gallbladder // VI Congress of Moscow Surgeons “Emergency and Specialized Surgical Care”. Congress materials. June 10-11, 2015 Moscow, Moscow: Alt Consul Publishing House, 2015 – pp. 71 – 72.
- Pat. 2013117186 RF MPK8 A61 B17/02. A method of temporary fixation of abdominal and pelvic organs during laparoscopic operations and a device for its implementation / K.V. Puchkov, V.V. Korennaya, D.K. Puchkov. - No. 2013117186/14; application 04/15/2013; publ. 10/27/2014, Bulletin 30.
- Puchkov K.V., Khubezov D.A., Puchkov D.K., Rodimov S.V. Minimally invasive laparoscopic methods for treating gallbladder diseases: a textbook for surgeons // Ryazan State Medical University of the Ministry of Health of Russia. - Ryazan: RIO RyazGMU, 2015. - 115 p.
- Puchkov K.V., Puchkov D.K. Comparative aspects of the use of a single laparoscopic and traditional laparoscopic approach in the treatment of simultaneous diseases of the abdominal organs // Moscow Surgical Journal. – 2015. – No. 2. – P. 17-20.
Puchkov K.V., Khubezov D.A., Puchkov D.K., Rodimov S.V. Minimally invasive laparoscopic methods for treating gallbladder diseases: a textbook for surgeons // Ryazan State Medical University of the Ministry of Health of Russia. - Ryazan: RIO RyazGMU, 2015. - 115 p.
Puchkov K.V., Puchkov D.K. SURGERY FOR GALLSTONES: laparoscopy, minilaparoscopy, single port, transanal access, simultaneous operations.-M.: ID "MEPRACTIKA-M", 2021, 312 p.
Watch a video of operations performed by Professor K.V. Puchkov. You can visit the website “Video of operations of the best surgeons in the world.”
Why do they trust us and choose the CELT clinic?
- CELT surgeons were among the first in the Soviet Union to begin performing laparoscopic gallbladder removal operations in 1991 in Moscow.
- CELT has accumulated experience in the treatment of complicated and acute forms of cholecystitis, and has developed methods for eliminating various complications and postoperative treatment tactics.
- Over 25 years of work, the permanent surgical team has successfully performed more than 15,000 endoscopic operations.
- Over the past 20 years, there has not been a single case of conversion (transition from laparoscopic to abdominal surgery in complex cases). Global statistics – 3-8%.
- Comfortable stay without pain during surgery and in the postoperative period.
- About 75% come to us for gallbladder removal surgery on the recommendation of their friends or relatives
Open cholecystectomy
This is a traditional abdominal surgery for gallstone disease, which is performed through a large incision on the body. It is performed in cases where there are contraindications to other types of cholecystectomy, as well as in acute inflammation of the gallbladder. The rehabilitation period takes about a month, sometimes more.
In some cases, surgeons at Clinic No. 1 in Khimki can perform cholecystectomy from a mini access only 3-5 cm long.
Doctors performing gallbladder removal

Lutsevich Oleg Emmanuilovich
Chief Surgeon of CELT, Honored Doctor of the Russian Federation, Chief Specialist of the Moscow Department of Health in Endosurgery and Endoscopy, Corresponding Member of the Russian Academy of Sciences, Head of the Department of Faculty Surgery No. 1 of the State Budgetary Educational Institution BPO MGMSU, Doctor of Medical Sciences, Doctor of the Highest Category, Professor
42 years of experience
Make an appointment

Gordeev Sergey Alexandrovich
Surgeon, Candidate of Medical Sciences, doctor of the highest category
41 years of experience
Make an appointment

Prokhorov Yuri Anatolievich
Surgeon, head of the surgical service of CELT, candidate of medical sciences, doctor of the highest category
32 years of experience
Make an appointment
Laparoscopic cholecystectomy
Laparoscopic cholecystectomy
is a surgical intervention that involves resection (removal) of the gallbladder using endoscopic equipment.
Today, this operation is the most common in the world among all laparoscopic manipulations and is a reliable method of combating gallbladder pathology. The surgical technique was developed and first used in Germany in 1882
and since then it has been constantly developed and improved.
Indications for cholecystectomy
- Cholelithiasis.
- Polyps (growths) on the inner walls of the gallbladder.
- Attack of acute cholecystitis (during the first 48 hours).
- Atypical (without a pronounced clinical picture) cholecystolithiasis (in the presence of a stone that threatens to block the bile ducts).
Contraindications for cholecystectomy
Absolute:
- Patient's agonal state.
- Violation of vital (vital) functions of the body.
- Pathology of blood clotting (congenital or acquired).
Relative:
- An attack of acute cholecystitis lasting more than 3 days.
- Pregnancy in the early (first trimester) and late stages (third trimester).
- Gallbladder atrophy. Acute infectious diseases.
- Hernial protrusions of the abdomen of considerable size.
- Some other conditions that, in the opinion of the anesthesiologist-resuscitator, prevent cholecystectomy.
Why does gallbladder pathology need to be treated surgically?
Constantly postponing or completely refusing surgery in patients for whom cholecystectomy is indicated routinely can result in serious complications. Gallstone disease can worsen at any time and cause an attack of severe hepatic colic, which not only becomes a source of pain, but is also a life-threatening condition.
Today, modern laparoscopic surgery is one of the most effective and safe methods of treating biliary tract pathology. Cholecystectomy allows the patient to be relieved of the root cause of the pathology, which is the key to a complete recovery from this disease.
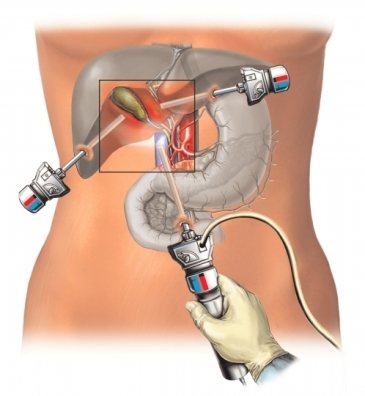
How is the operation performed?
Like most surgical procedures, laparoscopic cholecystectomy is performed under general anesthesia. Today, preference is given to spinal anesthesia options. The advantage of this method is that it has less impact on the central nervous system, which allows patients to endure anesthesia as gently as possible.
After complete anesthesia, endoscopic instruments are inserted through the anterior abdominal wall using small punctures (up to 1 cm in diameter). They are equipped with video equipment so that the doctor can monitor the progress of the operation through special screens. Using this equipment, the surgeon remotely removes the gallbladder. The duration of the operation depends on the individual characteristics of the patient and the skill of the surgeon, but on average it takes no more than 1 hour.
Recovery period
The most important advantage of laparoscopic cholecystectomy is the reduction of the recovery period. Due to the fact that during the manipulation there are minimal injuries, the recovery process proceeds much faster, and previously common complications such as peritonitis, suppuration or bleeding practically do not occur.
After the patient has recovered from anesthesia, he is activated within several hours (he is allowed to walk around the ward and visit the restroom on his own). In the absence of complications, the patient is discharged 3–4 days after the surgical procedure.
The timing of restoration of work activity depends on the individual characteristics of the recovery period, but on average ranges from 1 to 2 weeks.
Differences between laparoscopic cholecystectomy and classical (laparotomy)
| Criteria | Laparoscopic cholecystectomy | Abdominal surgery – laparotomy |
| Surgical approach | Punctures up to 1 cm in diameter. | Incisions at least 10 cm long (for more convenient access for the surgeon to the required organ). |
| Operation duration | 40 min – 1 hour. | 1.5 – 2 hours. |
| Activation period | Immediately after surgery. | Within 2–4 days after surgery |
| Discharge time | 2 – 3 days after surgery. | 7 – 10 days after surgery. |
| Restoration of labor activity | After 1 – 2 weeks | After 2 – 4 weeks |
| Risk of complications | Low, since during the operation the tissues were minimally injured, which further reduces the risk of secondary infection. | High, which is due to large trauma to tissues and blood vessels. A large incision can serve as an entrance gate for pathogenic microflora and the development of secondary infection. |
Checked the article and commented
Zagorov Alexey Sergeevich
Surgeon, coloproctologist.
General medical experience more than 10 years
Reviews of doctors providing the service – Cholecystectomy
Hello.
I would like to share my impressions after 3 brilliantly performed operations by the surgeons of the Multidisciplinary Clinic of CELT Dr. Bronshtein, Yuri Anatolyevich Prokhorov and the chief surgeon of CELT, Oleg Emmanuilovich Lutsevich, and express my gratitude to them from the bottom of my heart for the wonderful... Read full review Alexander Markovich A
07.08.2020
Hello. I would like to share my impressions after 3 brilliantly performed operations by the surgeons of the CELT Multidisciplinary Clinic Dr. Bronshtein, Yuri Anatolyevich Prokhorov and the chief surgeon of CELT, Oleg Emmanuilovich Lutsevich, and express my gratitude to them from the bottom of my heart for the wonderful... Read full review
Alexander Markovich A
07.08.2020