Stoparthrosis
» Treatment methods
» Ultrasound of hand joints
Kholikov T.V.
July 22, 2021 4701
Ultrasound examination is the most popular and sought-after method for diagnosing injuries, arthrosis and inflammation of the wrist joint and hand. It quickly and accurately allows you to obtain information about the condition of both bone and soft tissues of the joints. Ultrasound of the hand joints makes it possible to identify pathology at an early stage of its development and prevent possible loss of hand function.
Treatment with us is profitable!
- 20 years of experience
in treating diseases of the joints and spine - All in 1 day
— diagnostics, consultation and we will begin treatment
- Doctor's appointment 0 RUB! until September 30th!
when treated with us - PROMOTION
Sign up for an examination
Cost
2000 rub.
Duration
15-20 minutes
Experience of specialists
10-17 years
- 15 years of experience
in treating diseases of the joints and spine - All in 1 day
— diagnostics, consultation and we will begin treatment
- Doctor's appointment 0 RUB! until September 30th!
during treatment with us
Sign up for an examination
Old price:
duration
— a course of treatment
The advantage of the study is harmlessness, absence of contraindications, high reliability and accessibility. Diagnostics can be carried out over time, including for pregnant women, newborns and the elderly.
|
|


Ultrasound of the hand: what does the diagnosis show?
Ultrasound examination allows you to study the structure of muscles, ligaments, tendons, as well as assess the condition of cartilage tissue, fibrous capsules of joints, the quantity and quality of synovial fluid (the presence of pathological inclusions and fibers). The examination is carried out according to standard methods, which allows for a detailed study of all parts of the hands. Ultrasound of the hand joints helps diagnose:
- Ligament damage;
- Tendinitis;
- Arthritis of the hand;
- Carpal tunnel syndrome;
- Presence of neoplasms (hygromas);
- The presence of foreign bodies or hemorrhage into the joint cavity;
- Arthrosis of the wrist joint
Ultrasound of the joints of the hands in the specialized clinic “Stoparthrosis” allows the diagnostician to examine the smallest structures and give an accurate conclusion about the identified deviations from the norm.
The examination in the clinic is carried out using a highly sensitive device of the latest generation. Reception is carried out by qualified and experienced doctors, and if necessary, the clinic can consult an orthopedist, traumatologist or rheumatologist. Specialists will prescribe the necessary course of conservative medication or alternative therapy and monitor its effectiveness.
Sign up for an ultrasound of the hand joints
Author of the article:
Kholikov Timur Vyacheslavovich
Orthopedist
Make an appointment
Recent publications by the author:
- Ultrasound of hand joints
- Where to get an ultrasound of the knee joints?
- Ultrasound of the coccyx and sacrum
- What does ultrasound of soft tissues show?
What symptoms require an ultrasound examination?
- soreness in the hand;
- change in appearance, deformation of fingers or the entire limb;
- change in skin color;
- creaking in joints;
- local or general increase in temperature;
- swelling of the entire hand or a separate part;
- the appearance of neoplasms;
- inability to move your arm and perform usual actions;
- fracture, crack of bones or joints of the hand;
- sprain, rupture of ligaments;
- inflammation of tendons, soft tissues.
Ultrasound is also used in the examination of general diseases (endocrine, autoimmune) with damage to joints and bones, abscesses, arthritis and arthrosis, bursitis (inflammation of the synovial bursa of the joint).
FAQ
- Is it painful to have an ultrasound examination?
No, this is a non-invasive and painless diagnostic method.
- Will ultrasound be enough to make a diagnosis?
It all depends on the disease; for some diseases, only an ultrasound is sufficient, while others will require a more in-depth examination, such as magnetic resonance imaging or blood tests.
- Does ultrasound replace radiography of the joint?
No, ultrasound does not make it possible to assess the nature of the bone fracture, the presence of fragments and displacement. Therefore, in case of injuries and suspected fracture, it is better to first conduct an X-ray diagnosis.
- How is ultrasound of joints and soft tissues performed?
Everything is extremely simple: the doctor applies a special gel to the area under study, this gel helps ultrasound penetrate the tissue, and with the help of a sensor examines the tissues and processes occurring under the skin.
- How often can an ultrasound be done?
The ultrasound diagnostic method is absolutely harmless; if necessary, it can be done as many times as necessary.
- Is it possible to consult a specialist after an ultrasound?
Yes, you can get advice from a specialized specialist - a traumatologist, orthopedist, physiotherapist or sports doctor. You can also undergo treatment with us, and you can start on the same day you contact us.
- Do I need to somehow prepare for an ultrasound diagnosis of a joint?
No special preparation is required for ultrasound examination of joints and soft tissues. A contraindication to an ultrasound examination may be the presence of a plaster cast, wound or abrasion.
Normal ultrasound anatomy of the hand

Ultrasound scanner HS50
Affordable efficiency.
A versatile ultrasound scanner with compact design and innovative capabilities.
In recent years, all economically developed countries have seen an increase in injuries, in the structure of which injuries to the hand, due to its special functional significance in human production, occupy the most important place. A large proportion of diagnostic errors (21%), poor functional treatment outcomes are associated not only with the severity of injuries and diseases, the subtlety of the physiological function of the hand, the complexity of the anatomical structure, but also with the problem of identifying the pathology of the soft tissue structures of the hand [1-3]. In this article we want to highlight aspects of the normal ultrasound topographic anatomy of the hand, without knowledge of which it is not possible to make a correct diagnosis.
Ultrasound examinations of the soft tissue structures of the hand, which include tendons, nerves, and ligaments, are performed using ultrasound scanners equipped with multifrequency linear sensors with a frequency of 7 to 17 MHz, which ensures optimal visualization of the formations under study. The patient is seated opposite the examiner so that the hand is placed on the table. It is necessary to sequentially scan the dorsum of the hand from its proximal to distal parts, then the palmar surface in the same sequence. In case of hand pathology, it is necessary to specifically study the damaged area and compare it with the contralateral side. The condition of the tendons is assessed using dynamic echography in real time, during which the sliding movements of the tendon fibers are reproduced.
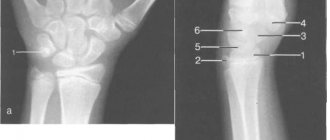
When scanning the dorsal surface of the distal third of the forearm and wrist joint, it is necessary to evaluate the condition of the extensor tendons, the triangular fibrocartilaginous complex (it looks like a triangular structure with mixed echogenicity, with the tip directed outward), carpal bones, scapholunate ligament and other small hand structures.

Rice. 1.
Ultrasound probe placement when examining the dorsum of the wrist and extensor tendons.
On the dorsum of the hand there are six fibrous canals of the extensor tendons of the fingers. By transversely scanning the dorsum of the wrist (sensor position is shown in Fig. 1), all anatomical structures in this area can be consistently visualized (Fig. 2).

Rice. 2.
Transverse echogram of wrist extensors. On the ulnar side there is a sixth pocket with the ulnar tendon of the extensor carpi (EC) and is easily visualized in the recess of the ulna. The fifth pocket contains the extensor digitorum (RM) and the fourth pocket contains the extensor digitorum flexor (EDC) and the extensor digitorum II (RIIP). The tendon of the third pouch (long extensor of the first finger - RIP) is located in close proximity to Lister's tubercle. The tendons of the second pouch are the long and short ones (DLRK and KLRK), the extensor radialis of the hand and the first pocket are the short extensor of the first finger, the LLR and the tendon of the muscle that abducts the first finger (OIP).
The first canal is located on the outer surface of the radius, it contains the tendons of the short extensor of the first finger and the long abductor muscle of the thumb. The tendon of the abductor digitorum muscle can be traced from the place of its attachment to the nail phalanx, while the tendon of the short extensor digitorum brevis is identified along the dorsal surface of the base of the proximal phalanx. The tendons of these two muscles are surrounded by a common tendon sheath.
The second canal is located lateral to the dorsal tubercle of the radius and contains the tendons of the long and short extensor carpi radialis.
In the third channel, the long extensor tendon of the first finger is visualized, which is located in close proximity to Lister’s tubercle. This anatomical feature causes spontaneous tendon rupture in a number of systemic diseases, in particular rheumatoid arthritis.
The fourth canal is located along the inner edge of the radius and the distal radioulnar joint and contains four tendons of the common extensor digitorum and one tendon of the extensor digitorum propria. The tendons have a common synovial sheath that reaches the middle of the metacarpal bones. Moving onto the hand, at the base of the proximal phalanx, from the II to V fingers, each tendon ends in a tendon extension that fuses with the articular capsule of the metacarpophalangeal joint. Tendon sprains are divided into three legs, of which the lateral ones are attached to the base of the distal phalanx, and the middle one is attached to the base of the middle phalanx.
More laterally, along the recess of the radioulnar joint, there is a fifth canal with the extensor tendon of the fifth finger. Coming out of the canal, the tendon of the little finger connects with the extensor tendon of the digitorum, which goes to the little finger, and together with it is attached to the base of the distal phalanx.
The sixth fibrous canal is visualized along the posterointernal surface of the head of the ulna in its groove. It contains the extensor carpi ulnaris tendon, surrounded by a synovial sheath and fixed to the fifth metacarpal bone.
An anatomical “snuffbox” is formed between the first and third fibrous canals, the bottom of which is the scaphoid and trapezoid bones, the apex is the base of the first metacarpal bone, and the base is the outer edge of the radius. The radial artery and the superficial branch of the radial nerve pass through the described gap. While visualization of the radial artery is not difficult for the examiner, the superficial branch of the radial nerve is so small that assessing its structure is often impossible.
The next important anatomical formations on the back of the hand, from the point of view of the potential for the development of pathology, are the scapholunate joint and the scapholunate ligament. Examination of the scapholunate ligament begins in the distal forearm so that the sonographic image includes both bones (radius and ulna). The probe is then slowly moved distal to the radioulnar joint until the three carpal bones are included in the projection: triquetrum, lunate, and scaphoid. While maintaining the transverse direction of the ultrasound sensor, the examination is moved to the radial side of the wrist (towards the first finger of the hand) in order to fully visualize the scaphoid and lunate bones. Ultrasound devices with high-resolution sensors visualize the scapholunate ligament, which lies in the form of a hyperechoic strip between these bones (Fig. 3).
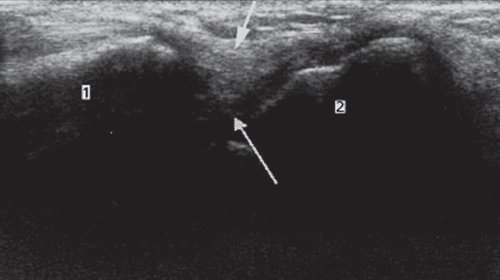
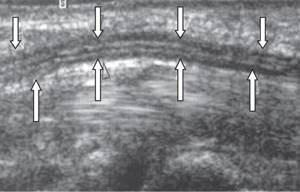
Rice. 3.
Transverse sonogram showing the scapholunate ligament (short light arrow), connecting the scaphoid (1) and lunate (2) bones.
When longitudinally scanning the dorsum of the hand (the position of the sensor is shown in Fig. 4, a), a sonographic assessment of the condition of the extensor tendons of the fingers and metacarpophalangeal joints is performed (Fig. 4, b).
Rice. 4.
Examination of the hand.

A)
The location of the ultrasound sensor when examining the dorsum of the hand (longitudinal scanning).
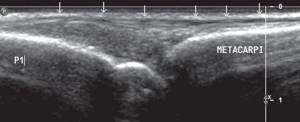
b)
Longitudinal sonogram of the extensor muscle of the third finger.
Metacarpi - metacarpal bone; P - main phalanx; arrows—extensor tendon.
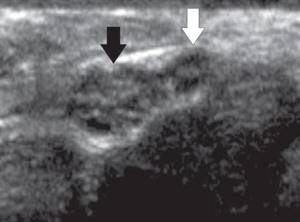
The structure of the extensor tendons must also be determined by transverse scanning of the dorsum of the hand in the area of the heads of the metacarpal bones (the position of the sensor is shown in Fig. 5, a). On the transverse sonogram, a rounded hyperechoic formation is clearly visualized - the extensor tendon of the finger and thin hypoechoic stripes that correspond to the collateral ligaments (Fig. 5, b).
Rice. 5.
Examination of the hand in the area of the metacarpal heads.

A)
The location of the sensor during transverse scanning of the dorsum of the hand in the area of the heads of the metacarpal bones.
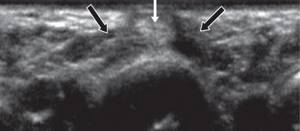
b)
Transverse sonogram of the dorsal surface of the metacarpophalangeal joints.
In the area of the heads of the metacarpal bones, a rounded hyperechoic formation is visualized - the extensor tendon of the finger (light arrow) and thin hypoechoic stripes that correspond to the collateral ligaments (dark arrows).
After examining the dorsum of the hand, we proceed to ultrasonography of the palmar surface.
When transversely scanning the palmar surface of the wrist joint (the position of the sensor is shown in Fig. 6), the flexor tendons, medial and ulnar nerves, and the radial and ulnar vascular bundles are visualized (Fig. 7).

Rice. 6.
The location of the ultrasound sensor when examining the palmar surface of the wrist and flexor tendons (transverse scanning).
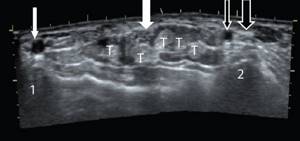
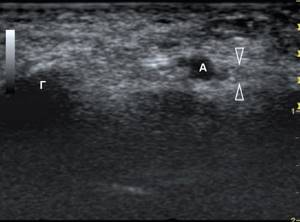
Rice. 7.
Transverse sonogram of the palmar surface of the wrist joint.
White arrow (thick)—median nerve; white arrow (thin) - radial artery; black arrow (bold)—ulnar nerve; black arrow (thin) - ulnar artery; T - flexor tendons of the fingers; 1 - radius; 2 - ulna.
There are four groups of flexor tendons in the distal wrist, each of which must be examined separately.
The flexor carpi radialis is the most lateral of all the flexors of the forearm. Its tendon passes under the flexor retinaculum to the base of the palmar surface of the second metacarpal. The palmaris longus muscle lies under the skin medial to the flexor carpi radialis. On the palmar surface of the hand, the muscle passes into a wide palmar aponeurosis, which is especially well developed in the middle of the palm, where it has the shape of a triangle with the base facing the fingers.
The largest group includes the deep and superficial digital flexor tendons and the flexor pollicis longus tendon, which are located within the carpal tunnel.
The carpal tunnel is one of the fibroosseous tunnels. Its medial bony border is formed by the hamate and triquetrum bones; the lateral bony border is the scaphoid. A thin fibrous ligament (flexor retinaculum), which is usually clearly visible on ultrasound, forms the roof of the carpal tunnel. The flexor pollicis longus tendon is located closer to the radial surface of the canal and has its own synovial sheath, the remaining eight flexor tendons are enclosed in a common tendon sheath. The tendons of the superficial flexor of the II-V fingers are covered in front by the flexor carpi radialis and the palmaris longus muscle, pass through the carpal canal and then each tendon is attached, respectively, to the base of the middle phalanges of the II-V fingers. At the level of the proximal phalanges, the tendon is divided into two legs, which are fixed to the lateral surfaces of the middle phalanges of the fingers. The deep flexor tendons of the II-V fingers are located in the carpal tunnel under the superficial flexor tendons. On the palmar surface of the fingers, each of the deep flexor tendons passes between the legs of the superficial flexor tendons of the fingers, attaching to the bases of the distal phalanges of the II-V fingers. Unlike the superficial, which flexes the main and middle phalanges, the deep flexor performs flexion of all three phalanges of the finger. The finger flexor tendons are fixed to the phalanges by means of the anular ligaments. The tendons of the superficial and deep flexor fingers have a common tendon sheath of the phalanges, without connecting to the common sheath. The exception is the synovial vagina of the fifth finger. When ultrasound examination is performed in a longitudinal projection, the structure of the tendons has a characteristic striation with parallel hyperechoic lines and a tubular structure.
When the sensor is shifted distally, the carpal ligament enters the scanning field, directly under which the median nerve is located. The nerve is easy to differentiate from surrounding tissues: it has a more ordered, “porous” structure, in contrast to the structure of tendons. In the area of the carpal canal, it is necessary to examine the structure of the nerve in both longitudinal and transverse projections (Fig. 8, a, b). Polypositional scanning data helps to correctly assess the structure of the median nerve and identify ultrasound signs of pathology.
Rice. 8.
Sonogram of the median nerve at the level of the carpal tunnel.
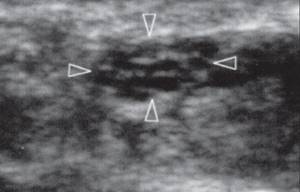
A)
Transverse sonogram of the median nerve at the level of the carpal tunnel; the nerve has a honeycomb-like structure with alternating hyper- and hypoechoic inclusions.
b)
Longitudinal sonogram of the median nerve (open arrows) at the level of the carpal tunnel. When scanning longitudinally, the nerve trunk is represented by a tubular structure with alternating hyper- and hypoechoic stripes.
The median nerve usually divides at its exit from the carpal tunnel and gives rise to the motor branch (Fig. 9) and the common digital nerves, which then end in the digital nerves proper. Digital nerves are accompanied by digital arteries, which can serve as a marker for ultrasound examination of these small structures. The diameter of the digital nerves is so small that their identification is only possible when using sensors with a frequency of at least 15 MHz.
Rice. 9.
Transverse sonogram of the median nerve (dark arrow) as it exits the carpal tunnel; branch of the motor branch (open arrow) of the median nerve.
When scanning the palmar-ulnar area of the hand at the level of the wrist joint, the best landmark is the ulnar artery, located outside the ulnar nerve. The flexor carpi ulnaris tendon occupies the most lateral position. Between the flexor tendons of the fingers and the tendon of the flexor carpi ulnaris there is a second osteofibrous tunnel of the palmar surface of the hand - Guyon's canal. It is formed by the transverse ligament, superficial palmar ligament, pisiform bone and hook of the hamate. The tunnel contains the ulnar artery and nerve, which at the exit from the canal are divided into deep and superficial branches (Fig. 10). The deep branch of the ulnar nerve is closely adjacent to the hamate bone, which can lead to
Rice. 10.
Transverse sonogram of the ulnar nerve (arrows) at the level of Guyon's canal.
A - ulnar artery; G - pisiform bone.
With transverse and longitudinal ultrasound scanning of the palmar surface of the hand, the condition of the metacarpophalangeal joints, palmar interosseous muscles, thenar and hypothenar muscles, the structure of the flexor tendons of the fingers, annular ligaments, common digital nerves, and palmar aponeurosis are assessed.
When transversely scanning the palmar surface of the hand at the level of the heads of the metacarpal bones (the position of the sensor is shown in Fig. 11), the tendons have an ovoid shape. Hypoechoic annular ligaments are located above the tendons. In the intermetacarpal space, lumbrical muscles and neurovascular bundles are located, and deeper - the palmar interosseous muscles (Fig. 12).
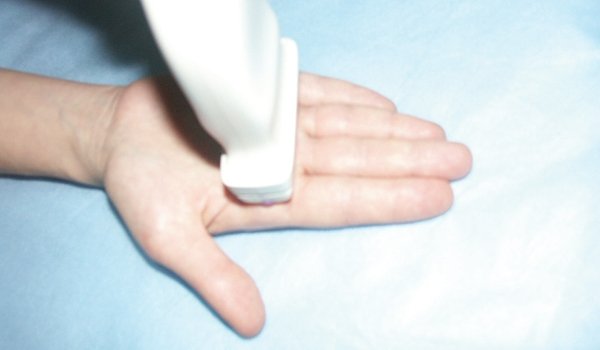
Rice. eleven.
The location of the ultrasound sensor when examining the palmar surface of the hand (transverse scanning).
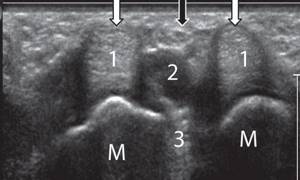
Rice. 12.
Transverse sonogram of the palmar surface of the hand.
M - heads of metacarpal bones; 1 - flexor tendons of the fingers; 2 - lumbrical muscles; 3 - palmar interosseous muscles; dark arrow—common digital nerve; light arrows—annular ligaments.
When longitudinally scanning the palmar surface of the hand (the position of the sensor is shown in Fig. 13), the tendons of the superficial and deep flexor of the finger and the metacarpophalangeal joint are visualized (Fig. 14).

Rice. 13.
The location of the ultrasound sensor when examining the palmar surface of the hand (longitudinal scanning).
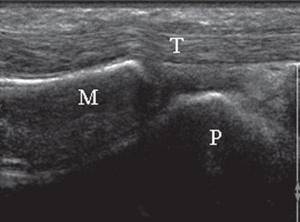
Rice. 14.
Longitudinal sonogram of the palmar surface of the hand.
M - metacarpal bone; P - main phalanx; T - flexor tendons of the fingers.
The standard position of the sensor when examining the thenar (eminence of the thumb) is shown in Fig. 15. This anatomical region is formed by the following structures: short abductor muscle of the first finger of the hand; muscle opposing the first finger of the hand; adductor pollicis muscle. It is quite difficult to differentiate each muscle using ultrasound. Against the background of the muscle mass, the tendon of the long flexor of the first finger is clearly visualized and, from a practical point of view, is of greatest interest (Fig. 16). As mentioned above, the tendon passes through the carpal tunnel, having a separate tendon sheath, and is inserted at the base of the distal phalanx of the thumb.

Rice. 15.
The location of the ultrasound sensor when examining the thenar muscles of the hand (longitudinal scanning).
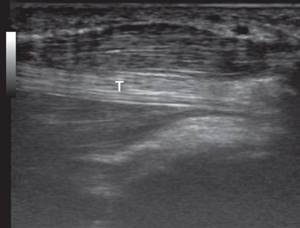
Rice. 16.
Longitudinal sonogram of the thenar hand.
T - tendon of the long flexor of the first finger.
Longitudinal examination of the fingers is optimal for assessing the flexor and extensor tendons. The flexor tendons are easier to examine with ultrasound scanning than the thinner extensor tendons. The superficial and deep flexor tendons are well visualized in the distal palm, but since they are located in the same synovial sheath, their differentiation is difficult (Fig. 17).
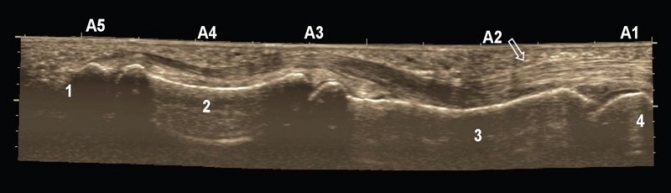
Rice. 17.
A panoramic sonogram of a longitudinal section of the deep and superficial flexor tendons at the level of the finger allows visualization of their attachments to the phalanges and the four pulleys (A). Block A2 (arrow) is best accessible for visualization.
1 - distal phalanx; 2 - middle phalanx; 3 - proximal phalanx; 4 - distal metacarpal bone.
When transversely scanning the palmar surface at the level of the proximal interphalangeal joint, the superficial and deep flexor tendons of the finger are easier to distinguish from each other - the deep flexor tendon has a structure of lower echogenicity (Fig. 18). By changing the position of the ultrasound sensor, it is necessary to achieve good visualization of the place of attachment of the superficial flexor muscle to the middle phalanx of the finger and the place of attachment of the deep flexor muscle to the distal phalanx. It should be remembered that when examining tendons in a longitudinal projection, one should try to position the sensor strictly perpendicular to the longitudinal axis of the tendon in order to more clearly visualize its structure and avoid the anisotropy effect. Depending on the anatomical site, a perpendicular position of the sensor to the tendon under study can be achieved by rocking the sensor forward and backward, right and left. Dynamic ultrasound examination helps to form a correct idea of the absence or presence of pathology. The researcher makes passive movements (flexion and extension) of the fingers, while the sliding movements of the corresponding tendons are clearly visible on the monitor screen.
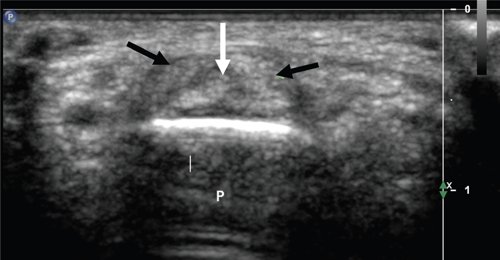
Rice. 18.
Transverse sonogram of the palmar surface of the finger at the level of the proximal interphalangeal joint.
P - main phalanx; dark arrows—pedicles of the superficial flexor tendon; light arrow—tendon of the deep flexor digitorum.
Longitudinal scanning of the palmar surface of the finger also allows one to evaluate the structure of bone formations: the contours of the main, middle and distal phalanges of the fingers, the articular surfaces of the distal and proximal interphalangeal joints, and the integrity of the lateral collateral ligaments. Of course, ultrasound scanning cannot replace traditional X-ray examination in diagnosing bone pathology, however, sonography can provide information about the condition of the cartilage, the integrity of the cortical layer and the ligamentous apparatus.
In conclusion, it should be noted that in the literature there are few publications devoted to the ultrasound anatomy of the hand. At the same time, knowledge of normal topographic anatomy and the effective use of sonography play an important role in making the correct diagnosis, which helps clinicians in determining treatment tactics. We hope that the material presented in our work will help specialists make wider use of the ultrasound method in studying the structures of the hand.
Literature
- Goloborodko S.A., Andruson M.V., Goridova L.D. Clinical diagnosis of motor disorders in chronic injuries of the median and ulnar nerves // Orthoped., trauma., prosthetics. 1985. N 10, pp. 27-30.
- Gorbatenko S.A., Eskin N.A. Ultrasound semiotics of lesions of the musculoskeletal system // Ultrasound and X-ray computed tomography. Prospects for development, possibilities of complex use with other diagnostic methods. M.: 1991. S. 27-31.
- Kovanov V.V., Navrotskaya V.V., Andreev I.D. Topographic anatomy of the upper limb // Operative surgery and topographic anatomy / Ed. Kovanova V.V. M.: Medicine. 1985. pp. 4-35.
Ultrasound scanner HS50
Affordable efficiency.
A versatile ultrasound scanner with compact design and innovative capabilities.
Our doctors
- LITVINENKO Andrey Sergeevich
Traumatologist orthopedist Sports medicine doctor Experience: 19 yearsSign up
- SKRYPOVA Irina Viktorovna
Physiotherapist rehabilitator Experience: 20 yearsSign up
- MOISEENKO Alexey Yurievich
Traumatologist orthopedist Sports medicine doctor Experience: 17 yearsSign up
- KHOLIKOV Timur Vyacheslavovich
Traumatologist orthopedist Sports medicine doctor Experience: 19 yearsSign up
Benefits of Ultrasound
Ultrasound of the veins of the upper extremities in comparison with other techniques is characterized by many advantages:
- does not cause pain;
- does not violate the integrity of the skin;
- has a favorable safety profile, since it does not expose the body to radiation and can be performed an unlimited number of times;
- has no contraindications and age restrictions;
- does not require preliminary preparation;
- allows you to quickly get results.
Why do they contact us?
- No queues
No need to wait, we work by appointment
- All in one day
Doctor's appointment, diagnosis and treatment on the day of treatment
- Let's relieve the pain
We will help you relieve pain in just 1-2 visits to us
- We guarantee
Professional approach, affordable prices and quality
- Doctor's appointment 0 RUB!
During course treatment all consultations are free
- Three treatment options
We will select several options and offer optimal treatment
results
The diagnostician records the detected violations in the area under study in detail in the protocol. With this document, the patient must go to an appointment with an orthopedist, where a further decision on treatment tactics will be made. In his conclusion, the ultrasound doctor does not make a diagnosis, but only describes in detail all the anomalies. The final diagnosis is made only by the attending physician, based on the anamnesis, the results of all studies, and only he makes a decision on further treatment.
There are 3 main factors as the cause of the disease (rheumatological triad)
- Genetic predisposition
- Hereditary tendency to autoimmune reactions
- More common in carriers of a certain MHC II class antigen: HLA - DR1, DR4
- Infectious factor
- paramyxoviruses - mumps, measles, respiratory syncytial infection viruses
- hepatoviruses - hepatitis B virus
- herpes viruses - herpes simplex viruses, herpes zoster, Cytomegalovirus, Epstein-Barr virus
- retroviruses - T-lymphotropic virus
- Triggering factor (hypothermia, hyperinsolation, intoxication, mutagenic medications, endocrinopathies, stress, etc.). For women, breastfeeding for a longer period of time reduces the likelihood of developing RA. Breastfeeding for 24 months or longer reduces the risk of developing RA by half.
What parameters are noted in the soft tissue ultrasound protocol?
When performing ultrasound diagnostics, pay attention to:
- exact location of the pathology,
- depth and size of the pathology.
- the structure of the neoplasm and surrounding tissues,
- blood supply to tissues.
Information about the blood supply to the problem area can indicate the nature of the pathology. For example, an ultrasound can detect a benign tumor - a lipoma, which is formed from adipose tissue. A lipoma has no blood supply, which makes it different from a malignant tumor. To clarify this point, patients are prescribed Dopplerography of the vessels of the problem area.
The exact location and size of the pathology must be known to the surgeon before the operation. In case of its deep location, patients are additionally prescribed MRI. When examining lymph nodes, attention is paid to their size, echogenicity and shape. In normal condition, the size of the lymph nodes should not exceed 1 cm. Their increase may indicate an inflammatory process in the body or infection.
Duration of the ultrasound procedure of the arteries and veins of the hands
A hand duplex scanning session lasts 20-40 minutes. The procedure is as follows:
- the subject sits or lies down on the couch;
- the doctor lubricates the device’s sensor with a special gel and begins an examination from the armpit area to the hand;
- during the ultrasound, the sonologist can squeeze the patient’s forearm or shoulder to speed up the movement of blood through the veins;
- the received information is displayed as a picture on the scanner screen.
Sometimes examining one limb is sufficient, but most often both arms are examined.

Hand ultrasound procedure
Indications for ultrasound of the shoulder joint
An ultrasound of the shoulder joint is prescribed if:
- constant pain and problematic movements in the shoulder area;
- injury or pathology detected by another method;
- the initial stage of a disease of the musculoskeletal system, which cannot be determined by a conventional x-ray;
- muscle pain;
- the need to determine the volume of effusion before puncture.
What does ultrasound show?
Ultrasound of the shoulder joint, what can be detected:
- Inflammatory processes - bursitis. Characteristic signs of this condition are changes in the size of the joint capsule and qualitative changes in its walls.
- Tendinitis is an inflammation affecting the ligamentous apparatus. In this case, a hyperechoic cord is determined at the site of injury.
- Shoulder fractures, which are characterized by a violation of the structural integrity of the bone tissue.
- Damage to the labia.
- Diagnostic symptoms of rheumatoid arthritis in the form of erosions of irregular shape and effusion into the cavity of the damaged joint.
Preparation for ultrasound of arteries and veins of the hands
Doppler ultrasound is a non-invasive research method that does not require complex preparation. The day before the procedure, heavy physical activity should be avoided. It's important to get a good night's sleep.
In order for the diagnosis to be reliable, it is necessary to stop using substances that can affect the condition of blood vessels:
- tobacco;
- alcohol;
- coffee;
- tea;
- energy drinks.
It is recommended to have a light snack before visiting the clinic. Creams and other cosmetics should not be applied to the skin of the hands.

Before a vascular ultrasound, you should give up coffee