Laboratory studies of biological fluids, such as blood and urine, make it possible to identify incipient pathologies at a very early stage of development. General (clinical) urine analysis is the most common, accessible and informative method used in medicine. Based on the data from this study, a specialist can assume the presence of a disease, which means conducting additional examinations and prescribing appropriate treatment.
A bad test result, that is, one that has deviations from generally accepted norms, causes slight panic, especially if it is the result of a urine test on an infant or small child. A poor urine test may be based not only on developing pathology of the kidneys or urinary system, but also on a number of other, often harmless, factors. At this moment, you need to put aside panic and listen to the observing/treating specialist.
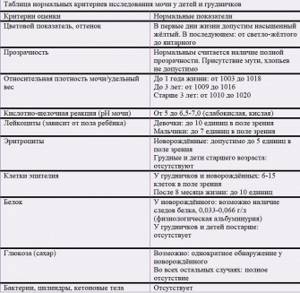
Norm
In infants and older children, the body functions a little differently than in adults. For example, in newborn babies the kidneys are relatively larger than in adults, they are located slightly lower and can be easily felt by palpation. The functionality of the kidneys is higher, which is associated with intensive metabolic processes.
The bladder has a smaller volume, and the mucous membrane of the urinary organs is easily damaged, which facilitates the penetration of pathogenic agents.
The urine of a newborn baby, in the first few days after birth, has a more saturated color. Physiological proteinuria (albuminuria), that is, the presence of protein in a urine test, is considered an acceptable phenomenon. During this same period, more uric acid may be present. Infants have an acid-base reaction, that is, the pH of urine, first sharply acidic and then weakly acidic.
The specific gravity also differs. In infants, the relative density of urine is relatively high, 1006-1018, then the indicators decrease to 1003-1005. Gradually, as the child grows older, the specific gravity of urine increases and reaches 1009-1016.
Causes
The first “bad test” is not a 100% reason for making a diagnosis. If deviations appear in the results, the specialist will prescribe a repeat general analysis. The form will contain the note “Cito!”, which means urgently, quickly. An exception will be the situation when the presence of pronounced symptoms of the disease is noted or the level of leukocytes/protein/red blood cells and other indicators is very high, in this case, a control analysis is carried out during treatment.
Physiological
An increase in the level of leukocytes or cloudy urine in a child does not always indicate the development of a pathological process in the body. There may be a number of natural, fairly easily removable reasons for such changes:
- Ignoring the conditions and rules for collecting urine. This should include poor washing of the child, the use of non-sterile containers for collecting a portion of biomaterial, incorrect collection process and long-term storage of urine (more than 2 hours). It is prohibited to use cotton wool, a diaper, or a diaper to collect urine from children. A modern, convenient and effective way would be to use special children's (pediatric) disposable urine bags, which are freely sold in pharmacies.
- Type of child’s nutrition, mother’s nutritional characteristics (during breastfeeding). For example, a large amount of protein foods in the diet of a mother or child can lead to the appearance of protein in the urine. Dehydration, that is, a lack of water in the child’s body, can also worsen the indicators. This picture is often observed in the presence of vomiting and/or diarrhea in an infant.
- Teething.
- Previously suffered from acute respiratory viral infections or acute respiratory infections.
- Recent vaccination(s).
- Presence of diaper rash or heat rash in a child.
- Exudative-catarrhal diathesis is a special predisposition of the skin and mucous membranes to inflammation.
In the event that there was an influence of the above reasons, a re-analysis will be good. Otherwise, the basis of a poor analysis is a disease.
Pathological
- Diseases and pathologies of the urinary tract. This can be balanoposthitis (in boys), urethritis, cystitis, nephritis, pyelonephritis (increased leukocytes, there is protein), glomerulonephritis (increased leukocytes, there are red blood cells). In these cases, the urine loses transparency, sediment may appear, and the color of the urine changes (white, dark, red).
- Diseases of other organs and systems: diabetes mellitus, pneumonia, thyroid diseases (goiter, hypothyroidism), rheumatism, systemic lupus and others.
- Disruption of metabolic processes (protein, water-salt, etc.).
- A long period of increased body temperature of the child.
- The use of a number of drugs for treatment (antibiotics, immunosuppressants, iron supplements, etc.).
- The presence of inflammatory diseases of the genital organs in girls (vulvovaginitis, vaginitis, etc.).
Urinalysis according to Nechiporenko in an infant
Urinalysis according to Nechiporenko in children under one year of age: what does it show and what are the features of preparing for it? Is this test included in the list of mandatory ones when examining the kidneys and bladder in children? About children's medical tests - in an interview with pediatrician, neonatologist Tatyana Gennadievna Fetisova.
— Tatyana Gennadievna, what does the Nechiporenko test show in a baby?
— Urinalysis according to Nechiporenko is a laboratory method for studying the urinary system, which is based on counting the number of red blood cells, leukocytes and cylinders in 1 ml of urine. The results obtained make it possible to diagnose problems with the urinary tract, kidneys and bladder.
— When is a Nechiporenko test prescribed for an infant? And how can a baby pass a urine test according to Nechiporenko?
— This testing is practically not prescribed for infants, except in rare cases. When a doctor sees clinical problems with the urinary system, but cannot identify their cause based on the results of a general urinalysis, then the diagnostic search is narrowed and a urine assessment according to Nechiporenko is prescribed.

Memo for parents: urine collection algorithm according to Nechiporenko in children
How to prepare your baby and collect urine
| Problems with urine collection in infants
|
“It is precisely because of the difficulties in collecting biomaterial that the Nechiporenko analysis is not carried out in children under one year of age. Initially, it is impossible to correctly collect the baby’s urine and isolate the middle portion from it. But the research method itself is very informative and high-quality: its results clearly reflect the situation with the urinary system.
— Some pediatricians are convinced that the Nechiporenko analysis is outdated and uninformative. Is it so?
— In 25 years of my service, I have never seen the urine of infants tested according to Nechiporenko. Perhaps somewhere such an analysis is present in diagnosis and treatment, but, most likely, with violations of the rules for collecting biomaterial.
This test is not outdated, and it is necessary for examining older children who already understand well what their parents tell them and can do what they are asked to do.
— What do the results of the Nechiporenko analysis mean?
— We have already discussed that the analysis involves counting the cells of the wall (surface layers) of the organs of the urinary system, which indicate inflammation and disorders.
Analysis values: what is the norm for children
- red blood cells - up to 1500;
- leukocytes - up to 2000-2500;
- cylinders - up to 20.
The results of the examination should always be “read” by a doctor, even if the indicators are within the normal range. The reasons for exceeding permissible values and treatment tactics are also determined by a specialist.
Symptoms
Associated symptoms of diseases are not always noticeable. That is why it is recommended to regularly submit biomaterial for examination. A urine test is prescribed at 1 month of life, 3 months, 6 months, 12 months. From 1 year of age to 14 years, it is recommended to take urine samples every 6 months.
If a child has a bad urine test result, you should pay close attention to his behavior and well-being. The following symptoms may be present:
- The baby writhes his legs and cries while urinating.
- There is poor weight gain.
- The baby eats little and sucks poorly.
- There is a periodic increase in body temperature, and vomiting is possible.
- Older children may complain of pain in the lower abdomen and do not want to sit on the potty because “it hurts to pee.”
- Swelling and bruises under the eyes appear on the eyelids, face, hands.
- Complaints of headache, weakness, lethargy, the child refuses to eat.
- Frequent urination, urine changes color and becomes cloudy. Little urine is produced.
- The child gets tired quickly.
The combination of at least one of the above symptoms with a poor urine result will be the basis for a preliminary diagnosis.
How does renal hematuria occur?
A consensus on the pathogenetic process of this phenomenon has not yet been developed. Of course, red blood cells can end up in the urine only by passing through the capillary bed, so hematuria in the presence of renal pathology is always associated with mechanisms of damage to the capillaries of the glomeruli of the kidneys. If a patient has microhematuria, this means that red blood cells have bypassed the pores of the highly permeable basement membranes and ended up in the urine. Gross hematuria is often caused by necrosis of glomerular renal loops.
A more likely version, according to which red blood cells penetrate the capillary walls, is high pressure in the glomeruli of the kidneys. Due to high pressure, red blood cells easily change their shape and pass through the capillary walls. Also, permeability to erythrocytes is ensured by defects in basement membranes. This is typical for immunoinflammatory processes when the capillary walls are damaged.
Thus, the nature of hematuria is not fully understood, but it is important for doctors to know where it occurs: in the tubules or glomeruli of the kidneys. Thanks to the dysmorphism of red blood cells, which is clearly visible during phase-contrast microscopic examination, it becomes possible to understand what kind of hematuria we are dealing with (renal or extrarenal).

Got some free time?
Then use it! Get additional education!
Decoding
The attending physician should decipher the test results. This is his direct responsibility and prerogative. Parents are advised to ask a specialist what the results are. If the doctor talks about a “bad” analysis, you need to find out what exactly this means and what indicators are increased/changed.
An analysis that indicates an increase in the number of leukocytes, the presence of protein, the appearance of turbidity, a change in color, the presence of red blood cells, sugar and/or bacteria is considered bad. Making a preliminary diagnosis, as well as planning further examination and treatment, depends on the totality of changes in urine analysis. In addition, one should take into account the presence of possible symptoms, which can be pronounced or absent altogether (signs of deteriorating health are subtle).
Methods for diagnosing hematuria
When the process is asymptomatic, its diagnosis is difficult, but a preliminary diagnosis can be established using anamnestic data. For example, a patient may talk about a persistent pain syndrome in the past or dysuric phenomena with a rise in temperature.
It is always advisable to begin making a diagnosis with a detailed history. It is important to find out the moment of the “debut” of hematuria and the circumstances of its appearance. If it appeared in childhood, most likely it is the consequences of a hereditary disease. It is necessary to clarify with the patient whether hematuria is constant or occurs periodically, along with some underlying disease. Proteinuria is also of great importance, especially if it is constantly present in the urine: such a symptom indicates its renal nature.
In addition, it is necessary to:
- two-glass sample;
- examination of the external genitalia;
- taking a smear for microscopic examination;
- scraping for enterobiasis;
- vulvogram or urocytographic examination;
- Ultrasound.
To clarify the diagnosis, intravenous urography or renoscintigraphy is prescribed.