Physical development of children and somatoscopy educational and methodological material on the topic
Physical development of children and somatoscopy
Physical development is one of the indicators of the health status of the population.
For a complete picture of the health status of the younger generation, in addition to morbidity and demographic data, it is also necessary to study the leading criterion for the health of the child’s body - physical development.
The term “physical development,” on the one hand, denotes the process of formation and maturation of the child’s body, on the other, the degree of this maturation at each given period of time, i.e., it has at least two meanings. Based on this, physical development is understood as a set of morphofunctional and functional indicators. These indicators make it possible to determine the reserve of physical strength, endurance and performance of the body, i.e. reflect the potential or real capabilities of the body to perform physical work. Physical development is largely determined by hereditary factors (genotype), but at the same time its level after birth (phenotype) largely depends on living conditions, physical activity and many other factors.
The physical development of a growing organism is one of the main indicators of a child’s health. The more significant the impairments in physical development, the greater the likelihood of diseases occurring.
At the same time, subject to laws, physical development depends on a number of factors of a socio-economic, medical-biological and environmental nature. This allows us to consider physical development as an objective indicator of the sanitary and epidemiological well-being of the population.
The study of physical development is carried out simultaneously with the study of health status during in-depth medical examinations carried out in children's and adolescent institutions. The study of a child’s physical development begins with establishing his calendar (chronological) age. For each child examined, the exact age at the time of examination, expressed in years, months and days, must be determined. This is necessary due to the fact that the rate of change in indicators of physical development is not the same in different periods of a child’s life, therefore, taking into account the changing rates of development, age grouping is carried out at different intervals (“time steps”).
Further, the program of unified anthropometric studies includes the determination of a number of basic characteristics from the entire variety of morphological and functional characteristics. These include somatometric, somatoscopic and physiometric signs.
Somatoscopy is carried out to obtain a general impression of the physical development of the subject: the type of structure of the body as a whole and its individual parts, their relationship, proportionality, the presence of functional or pathological abnormalities. Somatoscopic examination is very subjective, but the use of uniform methodological approaches (and in some cases, additional instrumental measurements) allows us to obtain the most objective data.
Somatoscopy includes:
1) assessment of the condition of the musculoskeletal system: determination of the shape of the skull, chest, legs, feet, spine, type of posture, muscle development;
2) determination of the degree of fat deposition;
3) assessment of the degree of puberty;
4) assessment of the condition of the skin;
5) assessing the condition of the mucous membranes of the eyes and oral cavity;
6) examination of teeth and drawing up a dental formula.
Assessment of the condition of the musculoskeletal system. When examining the skull, the difference between the anteroposterior and transverse diameters is taken into account. According to this principle, the shape of the skull is divided into mesocephalic (medium-headed), dolichocephalic (long-headed) and brachycephalic (short-headed). During somatoscopy, attention is paid to the shape of the skull, the structure of the crown, thickening of the sutures, the protrusion in the area of the large fontanel, the shape of the back of the head, and the presence of asymmetry of the skull. Deviations from the norm with the general characteristics of the skull are also noted.
The shape of the chest is determined by examination in the sagittal and frontal plane. There are three types of chest: cylindrical, flat and conical. The cylindrical chest is the most common shape, ensuring optimal function of the thoracic organs. This shape of the chest is characterized by uniform truncation to the upper and lower apertures, an average inclination of the ribs, tight adherence of the shoulder blades to the chest (due to the pronounced curvature of the ribs at the back), the presence of an oval line limiting the chest in front and an epigastric angle approaching a right angle. A flat chest, as a normal variant, is often found in preschool children due to poor development of small muscles that form the muscular corset. In older age groups, a flat chest usually indicates the presence of pathological abnormalities in the musculoskeletal system or somatic diseases that cause asthenia in the body as a whole. This form of the chest is characterized by the absence of truncation to the upper and lower apertures, a significant inclination of the ribs (“the ribs are limply lowered down”), the shoulder blades are spaced from the chest (“wing-shaped shoulder blades”, “angel wings”), the line limiting the chest in front is almost straight, the epigastric angle is acute. A conical chest, as a normal variant, does not occur in childhood and adolescence. As a relative variant of the norm, it occurs in professional weightlifters (due to a highly raised diaphragm as a result of activities associated with heavy physical activity in a static position). In other cases, the conical shape of the chest is due to the presence of severe stages of pulmonary pathology or obesity. The conical chest is characterized by pronounced truncation towards the upper aperture and absence of truncation towards the lower one, minimal inclination of the ribs or its complete absence, the shoulder blades are very close to the chest, the line limiting the chest in front is oval with a convexity in the lower part, the epigastric angle is obtuse. Deformations of the chest - asymmetry, “chicken breast”, “shoemaker’s chest”, etc. can be a particular manifestation of a disease of the entire skeletal system or organs of the chest cavity. With rickets, thickening of the thoracic ribs at the border of the cartilaginous and bone parts can reach significant sizes - “rickets rosaries”.
When determining the shape of the legs, the examinee stands at attention. With the normal shape of the legs, they touch at the knee joints and inner ankles. X-shaped legs - the knee joints come one behind the other, and when the knee joints touch, the inner ankles are spaced apart. As a variant of the norm, this form is often found in preschool children. Subsequently, the legs, as a rule, acquire a normal shape. In obese people, the X-shaped legs are caused by increased fat deposition in the thighs. O-shaped legs - knee joints do not touch each other. This shape of the legs can be a manifestation of diseases of the skeletal system of various etiologies and, in particular, a sign of rickets. Rachitic deformities of the limbs are determined by palpating thickenings on the epiphyses in the form of bracelets; in addition, curvature of the thighs and legs (saber-shaped legs) can be observed.
To determine the shape of the foot, its supporting surface is examined and attention is paid to the width of the isthmus connecting the heel area to the front part and the location of the vertical axes of the Achilles tendon and heel under load. A normal foot has a narrow isthmus, the vertical axes are located along one line perpendicular to the surface of the support. Flattened foot - the isthmus is wide, the line of its outer edge is more convex, the vertical axes are perpendicular to the surface of the support. Flat foot - the isthmus occupies almost the entire width of the foot, the vertical axes of the heel and Achilles tendon form an angle open outward. To objectively assess the shape of the foot, the plantography method is used - obtaining an imprint and then calculating it.
The spine is examined in the sagittal and frontal planes. The presence of physiological curves of the spine in the sagittal plane is determined: cervical, thoracic and lumbar, which perform the function of shock absorption when walking, running and other movements. In the frontal plane, the spine is normally a straight line, the shoulders are at the same level, the shoulder blades are symmetrical, the waist triangles formed by the waist line and the lowered arm are equal to each other. In pathological conditions, curvature of the spine is possible. In the sagittal plane - lordosis (forward) and kyphosis (backward). At the same time, the physiological curves of the spine are enhanced, and it is also possible to smooth out the cervical and lumbar curves, and total kyphosis of all parts of the spine. Kyphosis of some parts of the spine entails the formation of lordosis in other parts and vice versa. The depth of the cervical and lumbar curves normally ranges from 3-5 cm, depending on the length of the spine. In the frontal plane - scoliosis, which can cover all parts of the spine (complete) and part of it (partial). Depending on the direction of the bending arc, right- and left-sided scoliosis is distinguished. With scoliosis, there is an asymmetry in the level of the shoulders, shoulder blades and waist triangles, and the presence of muscle compensatory ridges. Since the body requires a vertical position for balance, scoliosis in one part of the spine causes the development of the opposite scoliosis in another part. Lateral curvature of the spine is determined by the deviation of the line of the spinous processes of the vertebra from the vertical line to the right or left. I degree – functional disorders, unfixed, disappearing with active muscle tension. II degree – persistent curvatures that do not disappear with muscle tension. III degree – pronounced curvatures, accompanied by deformations of the chest or asymmetrical position of the pelvic bones. Combined curvatures of the spine in the frontal and sagittal planes (kyphoscoliosis) can be accompanied by compensatory lordosis and scoliosis, deformities of the chest, changes in the configuration of the pelvis and the symmetry of its location. Posture is the usual posture of a casually standing person, when the body and head are held straight, without active muscle tension. It depends on the shape of the spine, the uniformity of development and muscle tone, and may also be associated with age-related characteristics of the processes of growth and development and the acquired skills of maintaining the correct posture. Types of scoliosis: thoracic, general left-sided, S-shaped. Conventionally, all types of posture can be divided into 2 subgroups:
1. types of posture in which the cervical and lumbar sagittal curves of the spine are equal to each other or differ by no more than 2 cm: Correct - the cervical and lumbar curves do not exceed 3-5 cm, depending on the length of the spine, the head is raised, the shoulders are slightly abducted posteriorly, the chest protrudes slightly forward, the stomach is tucked. Straightened - all physiological curves are smoothed out, the back is sharply straightened, the chest protrudes noticeably forward. With a pronounced straightened posture, the shock-absorbing functions of the spine are disrupted, the gait changes, and activities associated with walking, sudden movements and physical efforts in an upright position of the body become difficult. Kyphotic - the cervical and lumbar curves are sharply increased, the head and shoulders are lowered, the stomach protrudes forward. Kyphotic posture is usually accompanied by curvature of the spine in the cervical and lumbar regions (lordosis) or in the thoracic region (kyphosis). Progression of the disease can lead to the development of total kyphosis of the cervical, thoracic and lumbar spine;
2. types of posture in which the difference between the cervical and lumbar sagittal curves of the spine exceeds 2 cm: Lordotic - the lumbar curve is sharply increased while the cervical curve is smoothed, the upper part of the body is slightly thrown back, and the stomach protrudes forward. This type of posture, as a relative variant of the norm, is observed in preschool children as a result of poorly developed muscles, especially small muscles that form the “muscle corset.” The detection of lordotic posture at older ages indicates the possible presence of somatic pathology that affects the physical development of the body as a whole. Stooped - the cervical curve is increased while the lumbar curve is smoothed, the head is tilted forward, the shoulders are lowered. Slouched posture is common in adolescence and is associated with a sharp increase in body length during the prepubertal period. To determine the type of posture, visual observations can be supplemented with instrumental research. To do this, measure the depth of the cervical curve (at the level of the spinous process of the VII cervical vertebra) and the depth of the lumbar curve (at the point of greatest bending).
Muscle development is characterized by the amount of muscle tissue and its elasticity; the shape of the chest, the position of the shoulder blades, and the shape of the abdomen are taken into account. Descriptive features are supplemented by measurements of muscle strength and the difference between shoulder circumferences in a free and tense state. I degree - poor muscle development - muscle relief is not expressed, elasticity is reduced, the chest is flat, the shoulder blades are not adjacent to the chest, the stomach is saggy, muscle strength is below average. II degree - average development of muscles - the relief of the muscles is somewhat marked, they have average elasticity, the chest is cylindrical, the angles of the shoulder blades may protrude somewhat, the stomach is tucked or slightly protrudes forward, muscle strength indicators are within average values. III degree - good muscle development - the muscles have a pronounced relief, are quite elastic and large in volume, the chest is cylindrical, the shoulder blades are tightly attached to it, the stomach is tucked, muscle strength is above average.
The degree of fat deposition is assessed visually by the severity of the bone relief and the thickness of the subcutaneous fat layer, by measuring the thickness of the skin-fat folds. For measurements, sliding compasses or calipers of various types are used. All measurements are taken on the right at four points: On the chest - vertically along the midclavicular line at the level of the 3rd rib. On the stomach - vertically 5 cm to the left of the navel. Under the scapula - at the lower edge of the angle of the scapula along the segmental line. On the shoulder - above the triceps in the middle of the shoulder along the line connecting the acromion (acromial process of the scapula) and olecranon (ulnar process of the ulna). The thickness of the skin-fat fold is estimated in mm. I degree of fat deposition - the bones of the shoulder girdle and ribs are sharply contoured, the thickness of the skin-fat folds is up to 5 mm inclusive. II degree of fat deposition - the bone relief is somewhat smoothed, the thickness of the folds is 6-9 mm. III degree of fat deposition - the bone relief is smoothed, the contours of the body are rounded, the thickness of the folds in children is 10-15 mm, in adults - up to 20 mm.
The degree of puberty is assessed by the level of development of secondary sexual characteristics. In girls, the following is determined: armpit hair, pubic hair, breast development, age at first menstruation. In boys, it is determined: armpit hair, pubic hair, voice mutation, facial hair, development of the Adam's apple. The level of development of traits is assessed and recorded according to a certain scheme.
The condition of the skin is assessed by the following external signs: Color - pink, pale, cyanotic, icteric, the presence of hyperemia of the general or partial, pronounced venous network. Pigment deposition - general, local (armpits, palms, other places). Focal changes in the color and surface of the skin - erythema, hemorrhages, peeling, stretch marks, various forms of eczema, purulent and ulcerative lesions. Elasticity - is examined by lifting the skin without subcutaneous tissue near the axillary cavity, on the lower part of the forearm or on the back of the hand: elastic - the fold disappears quickly, flaccid - the fold does not straighten out for a long time. Turgor is examined by squeezing the skin and all soft tissues on the inner surface of the thighs with your fingers: pronounced - resistance to compression is felt, reduced - resistance to compression is weakened. Humidity – dry, wet, profuse sweating. Hyper- and hypotrichosis. Postoperative and post-traumatic scars.
The condition of the mucous membranes is assessed by examining the lower eyelids of the eyes and gums. Their color is noted - pink, pale, moderate hyperemia, severe hyperemia, cyanotic, icteric, the presence of hemorrhages, or any plaque. Examination of teeth and drawing up a dental formula. Teething is a physiological act and an indicator of the level of biological development of the child. The eruption of baby teeth begins in the second half of life and ends by 2.5-3 years. The total number of milk teeth is 20. On the upper and lower jaws, on the right and left, 2 incisors, 1 canine, 1 small molar (premolars) and 1 large molar (molars) erupt, respectively. Early eruption of baby teeth - up to 4-4.5 months is a deviation from the norm and indicates a possible rickets (if this is not due to the genetic characteristics of the child's development). By the age of 12-13, all baby teeth fall out, leaving permanent teeth in the bite. The eruption of permanent teeth begins at 5-6 years of age and ends by 15-18 years. The 8th teeth may erupt at an older age or be absent altogether. The first molars erupt, then the incisors, first premolars, canines, second premolars, second molars, and then the 8th wisdom teeth. The total number of permanent teeth is 32. On the upper and lower jaws on the right and left, respectively, there are 2 incisors, 1 canine, 2 small molars, 2 large molars and 1 large wisdom molar. From the standpoint of age-related physiology and dentistry, 3 periods are distinguished in the change of teeth in children: the first - in young children (up to 2.5 years), the eruption of milk teeth with not yet formed roots occurs; second – in children aged 2.5 to 6 years, teething and the formation of their roots are completed; third - in children from 6 to 12 years old, the roots of baby teeth are reabsorbed and permanent teeth erupt, the roots of which are in the stage of formation. The corresponding milk and permanent teeth do not differ from each other in shape, but the milk teeth are smaller in size and by the time their roots are completely reabsorbed, they have worn incisal edges and chewing surfaces. Erupted permanent teeth are characterized by the presence of denticles along the edges of the incisors and pronounced tubercles on the surface of the small and large molars. During the examination, the number of teeth, primary or permanent, color, shape, position in the dental arch, and the condition of hard tissues are determined. Healthy (intact), carious, and filled teeth are identified. The results of the dental examination are entered into a special chart (dental formula). The horizontal line of this diagram indicates belonging to the upper or lower jaw, the vertical line - to the right or left half of the jaw. Milk teeth are designated by Roman numerals, permanent teeth by Arabic numerals. Instead of missing teeth, a “0” is entered, carious teeth are recorded with the mark “k”, and filled teeth are recorded with the mark “p”.
To study, analyze and evaluate the physical development of large groups of children or individuals, 2 main observation methods are used. The generalizing method (population cross-sectional method) is based on a one-time examination of the physical development of large groups of children of different ages. Each age group must consist of at least 100 people. The method is used on a large number of observations in order to obtain age-sex standards and assessment tables used both for individual assessment of physical development and for environmental and hygienic assessment of the area where children live. The method makes it possible to monitor dynamic changes in the physical development of children in a given region in connection with health status, physical education, living conditions, nutrition, etc. The individualizing method (longitudinal section) is based on an examination of a specific child, one-time or over the course of years, with subsequent assessment of its biological level of development and harmony of morphofunctional status using appropriate assessment tables, making it possible to obtain sufficient saturation of each age-sex group by month or year of life with a relatively small number of observations. This technique allows us to determine the characteristics of the physical formation of the body from month to month (or from year to year) of the observed group of children in a homogeneous population.
The individualizing method does not contradict the generalizing method and is a significant addition to it both in studying the process of general development of the child and in clarifying the influence of environmental factors during this development.
To obtain average indicators of physical development, large groups of practically healthy children of various age and sex groups are examined. The obtained average values are the standards of physical development of the corresponding groups of the child population.
External examination (somatoscopy)
When studying the physical development of a person, along with data obtained by instrumental methods, descriptive indicators are also taken into account.
The examination begins with an assessment of the skin, then the shape of the chest, abdomen, legs, degree of muscle development, fat deposits, condition of the musculoskeletal system and other parameters (indicators).
The skin is described as smooth, clean, moist, dry, elastic, flaccid, acne-prone, pale, hyperemic, etc.
The condition of the musculoskeletal system (MSA) is assessed by the general impression: massiveness, shoulder width, posture, etc.
Spine - performs the main supporting function (see Fig. Human skeleton). It is examined in the sagittal and frontal planes, the shape of the line formed by the spinous processes of the vertebrae is determined, attention is paid to the symmetry of the shoulder blades and the level of the shoulders, the state of the waist triangle formed by the waist line and the lowered arm (see Fig. Determination of spinal curvature).
Human skeleton
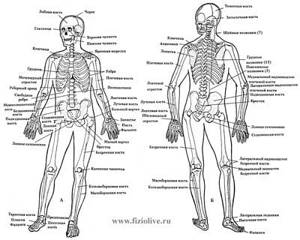
Human skeleton (a - front view; b - rear view)
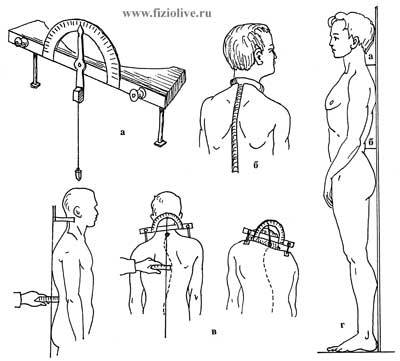
Determination of spinal curvature

Signs of normal posture (a); determination of spinal curvature (b). Types of scoliosis: 1 - right-sided; 2 - left-handed; 3 - S-shaped
A normal spine has physiological curves in the sagittal plane; the frontal view is a straight line. In pathological conditions of the spine, curvatures are possible both in the anteroposterior direction (kyphosis, lordosis) and lateral (scoliosis).
To determine the lateral curvatures of the spine, a Billy-Kirchhofer scoliosometer is used (see Fig. Lordosobrachial-scoliozometer).
Lordosobrachial-liozometer
Lordosobrachial-liozometer (a). Determination of lateral curvatures of the spine using the Billy-Kirchhofer device (b), lordobrachial coliozometer P.I. Belousova (c); d - diagram for measuring the depth of the cervical (a) and lumbar (b) curve
A flat back is characterized by smoothness of all physiological curves of the spine.
A rounded back (stooping) is a form of thoracic kyphosis.
With a round-concave back, thoracic kyphosis and lumbar lordosis are simultaneously increased.
With plano-concave, only the lumbar lordosis is increased.
Posture is the habitual posture of a casually standing person. It depends on the shape of the spine, the uniformity of development and tone of the torso muscles. There are correct posture, stooped, kyphotic, lordotic and straightened (see Fig. Types of posture). To determine posture, visual observations are made of the position of the shoulder blades, shoulder level, and head position. In addition, they include instrumental studies (determining the depth of the cervical and lumbar curves and the length of the spine).
Types of posture
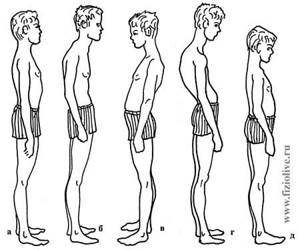
Types of posture: a - normal; b - stooped; c - lordotic; g - kyphotic; d - straightened (flat)
Normal posture is characterized by five signs (see Fig. Determination of spinal curvature; Normal posture):
1 - location of the spinous processes of the vertebrae along the plumb line, lowered from the tubercle of the occipital bone and passing along the intergluteal fold;
2 - placement of the shoulders at the same level;
3 — arrangement of both blades at the same level;
4 - equal triangles (right and left), formed by the torso and freely lowered arms;
5 - regular curves of the spine in the sagittal plane (up to 5 cm deep in the lumbar region and up to 2 cm in the cervical region).
Normal posture
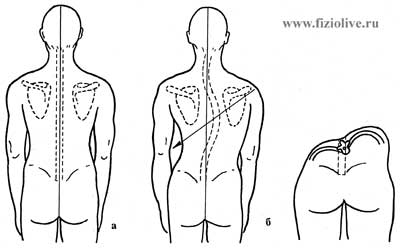
Normal posture (a), scoliosis (b)
With a number of diseases (scoliosis, kyphosis, etc.), a change in posture occurs (see Fig. Normal posture). Often, participation in the corresponding sport, early specialization (gymnastics, barbell, etc.) lead to dysfunction of the spine and muscle imbalance, which negatively affects the function of internal organs and the performance of a person as a whole.
When determining the shape of the legs, the examinee brings the heels together and stands straight. Normally, the legs touch at the knee joints; with an O-shape, the knee joints do not touch; with an X-shape, one knee joint overlaps the other (see Fig. Shape of legs).
Leg shape
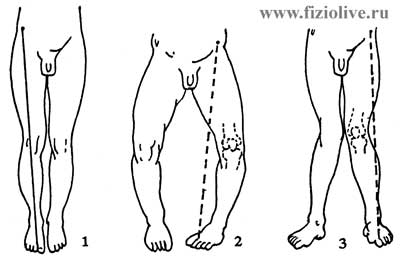
Leg shape: 1 - normal (the axis of the lower limb is normal); 2 — O-shaped deformity of the lower limb (varus); 3 - X-shaped (deformation of the lower limb (valgus)
The foot is an organ of support and movement. There are normal, flattened and flat feet (see Fig. Appearance of the feet and their prints). When examining the foot's supporting surface, pay attention to the width of the isthmus connecting the heel area to the forefoot. In addition, pay attention to the vertical axes of the Achilles tendon and heel under load.
Appearance of feet and their prints
The appearance of the feet and the imprints of their soles are normal (a) and with flat feet (b). Schematic representation of the bones of the foot normally (a) and with longitudinal flatfoot (b). Determination of the shape of the foot (c): a - width of the isthmus; a + b - width of the foot
In addition to the examination, you can obtain foot prints (plantography). The degree of flattening of the foot is calculated using the Strieter method (see Fig. Appearance of the feet and their prints).
Examination of the chest is needed to determine its shape, symmetry in breathing of both halves of the chest and the type of breathing.
The shape of the chest, according to constitutional types, is of three types: normosthenic, asthenic and hypersthenic. More often the chest is of mixed shape.
The normosthenic shape of the chest is characterized by the proportionality of the relationship between its anteroposterior and transverse dimensions; the supra- and subclavian spaces are moderately pronounced. The shoulder blades fit tightly to the chest, the intercostal spaces are not clearly defined. The epigastric angle approaches a straight line and is approximately 90°.
The asthenic shape of the chest is quite flat, because the anteroposterior size is reduced in relation to the transverse one. The supra- and subclavian spaces are sunken, the shoulder blades are spaced from the chest. The edge of the X rib is free and easily identified by palpation. The epigastric angle is acute - less than 90°.
Hypersthenic chest shape. Its anteroposterior diameter is more normosthenic, and therefore the transverse section is closer to a circle. The intercostal spaces are narrow, the supra- and subclavian spaces are poorly defined. The epigastric angle is obtuse - more than 90°.
Pathological forms of the chest develop under the influence of painful processes in the organs of the chest cavity or due to skeletal deformation. In athletes, funnel chest, rachitic, scaphoid, etc. are often found.
The shape of the chest can also be affected by various types of spinal curvature. Thus, kyphotic curvature of the spine is often combined with simultaneous scoliosis and is called kyphoscoliosis, and the chest is kyphoscoliotic.
When examining the chest, it is also necessary to pay attention to the type of breathing, its frequency, depth and rhythm. The following types of breathing are distinguished: chest, abdominal and mixed. If breathing movements are performed mainly due to contraction of the intercostal muscles, then they speak of the thoracic, or costal, type of breathing. It is characteristic mainly of women. The abdominal type of breathing is typical for men. The mixed type, in which breathing involves the lower chest and upper abdomen, is typical for athletes.
Muscular development is characterized by the amount of muscle tissue, its elasticity, relief, etc. Muscular development is additionally judged by the position of the shoulder blades, the shape of the abdomen, etc. Muscular development largely determines the strength, endurance of a person and the type of sport he practices.
The degree of sexual development is an important part of the characteristics of the physical development of schoolchildren and is determined by a set of secondary sexual characteristics: pubic and axillary hair, in addition, in girls - by the development of the mammary gland and the time of the appearance of menstruation, in boys - by the development of facial hair , Adam's apple and voice mutations.
The physique is determined by size, shape, proportion (the ratio of one body size to another) and the peculiarities of the relative arrangement of body parts. Body type is influenced by the type of sport, nutrition, environment (climatic conditions) and other factors. Constitution is the characteristics of a person’s physique. M.V. Chernorutsky distinguishes three types of constitution (see Fig. Body types): hypersthenic, asthenic and normosthenic. The author takes into account both morphological and functional characteristics of the individual.
Body types
Body types: a - asthenic; b - normosthenic; c - hypersthenic (M.V. Chernorutsky, 1938)
With a hypersthenic body type, the transverse dimensions of the body predominate, the head is round in shape, the face is wide, the neck is short and thick, the chest is wide and short, the stomach is large, the limbs are short and thick, and the skin is dense.
The asthenic body type is characterized by a predominance of longitudinal body dimensions. Asthenics have a narrow face, a long and thin neck, a long and flat chest, a small belly, thin limbs, underdeveloped muscles, and thin pale skin.
Normosthenic body type is characterized by a proportional physique.
A relationship has been noted between a person’s constitutional type and his susceptibility to certain diseases. Thus, asthenics are more likely to have tuberculosis and diseases of the gastrointestinal tract, while hypersthenics are more likely to have metabolic disease, liver disease, hypertension, etc.
Conrad (1963), based on morphological characteristics, distinguishes the following body types among athletes: leptomorph, ateltomorph, pycnomorph, metromorph (depending on the degree of manifestation of dolicho- and brachymorphism).
It should be noted that clearly defined body types among athletes are rare. More often there are various combined forms with a predominance of signs of one or another body type. However, there are characteristic body types for individual sports. Thus, basketball players are tall, weightlifters and throwers are massive, short people predominate in artistic gymnastics, etc.