Postcholecystectomy syndrome. Causes

diagnostic errors made before surgery and technical errors during surgery,- functional disorders associated with removal of the gallbladder,
- exacerbation of diseases existing before surgery, primarily pancreatic diseases,
- development of new conditions of the gastrointestinal tract in connection with removal of the gallbladder (bile reflux into the stomach, loose stools, disruption of food digestion processes).
Treatment of recurrent bowel cancer
If a relapse is diagnosed, medical tactics for oncological pathology are determined by the number of foci and their location. Operable local tumors are subject to repeated surgical removal. If surgery is not possible and the cancer has spread, chemotherapy is the treatment of choice. If the malignant process is limited to the pelvic area, radiation therapy is used.

Palliative surgical interventions are often performed in case of relapse. In case of intestinal obstruction, a colostomy is performed. Interintestinal abscesses are opened and drained. For single cancer metastases to the liver and lungs, radical excision is sometimes performed. More often, oncologists use combined treatment for relapse.
Functional disorders of the sphincter apparatus of the biliary tract
It is currently considered a proven fact that after removal of the gallbladder, there is an increase in the tone of the sphincter of Oddi, the reason for which is the exclusion of the regulatory role of the sphincter of the gallbladder and the muscular activity of the gallbladder on the sphincter of Oddi.
After removal of the gallbladder, mechanisms of adaptation to the functioning of the biliary tract without the gallbladder are activated. Changes in the motor function of the sphincter of Oddi are one of the reasons for the formation of acute or chronic abdominal pain and dyspeptic syndrome in the postoperative period. Restructuring of the biliary tract after cholecystectomy can last up to 1 year after surgery.
Dysfunction of the sphincter of the common bile duct and other sphincters of the biliary system can lead to increased pressure in the ducts, stagnation of bile in them, which is manifested by pain in the right hypochondrium or in the epigastric region. If dysfunction of the pancreatic duct predominates, then a clinical picture characteristic of pancreatitis appears.
The variety of clinical manifestations of PCES makes it difficult not only to determine the type of functional disorders of the sphincter apparatus of the biliary system, but also complicates the diagnosis of PCES.
Preventing cancer recurrence
To reduce the frequency of relapses of malignant intestinal pathology, doctors recommend adhering to the following rules:
- lead an active healthy lifestyle;
- eliminate bad habits, stress, carcinogenic factors;
- limit the consumption of alcoholic beverages;
- adhere to a rational, balanced diet, with a predominance of plant foods;
- control your weight.
After radical cancer treatment, you need to constantly prevent relapses by regularly visiting your oncologist for monitoring and following all his recommendations. In this case, the probability of a favorable outcome will be maximum.
Book a consultation 24 hours a day
+7+7+78
Disorders of the liver, pancreas and intestinal tract after cholecystectomy
Removal of the gallbladder rebuilds the processes of bile formation and bile excretion.
- There is an increase in bile production by the liver, which is the main cause of diarrhea after cholecystectomy. Taking choleretic drugs in these cases is undesirable!
- The most common area affected after gallbladder removal is the pancreas. In case of cholelithiasis, dysfunction of the sphincter apparatus of the biliary tract, impaired motor function of the gallbladder before surgery, chronic biliary pencreatitis is formed (pancreatitis, the cause of which is a violation of the bile secretion system).
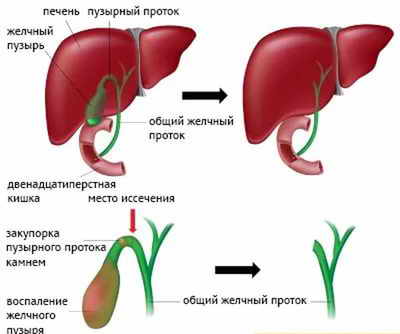
- Sometimes there are lesions of the ductal system that disrupt the outflow of bile - narrowing, stones in the ducts, enlarged lymph nodes, inflammatory diseases in the sphincter-ductal system.
As a result, exacerbations of chronic pancreatitis after removal of the gallbladder occur quite often - from 5 to 90%. This scatter is explained by the fact that sufficient examination was not carried out before the operation to assess the condition of the pancreas, but in some cases there is an overdiagnosis of chronic pancreatitis.
In medical practice, it is noted that the longer gallstones exist in the gallbladder, the more often chronic pancreatitis occurs.
In the pancreas, the volume of enzyme secretion decreases, exocrine pancreatic insufficiency develops, and digestive processes are disrupted. Cholecystectomy, performed on time, helps to improve or normalize the parameters of the enzymatic function of the pancreas.
After removal of the gallbladder, the function of the duodenum is often disrupted, which is confirmed by the appearance of duodenogastric reflux, i.e., the reflux of the contents of the duodenum into the stomach, causing morphological changes in the outlet of the stomach and the formation of chronic reflux gastritis (gall).
After removal of the gallbladder, the function of the small intestine (absorption of food components) and the motor function of the large intestine (constipation, diarrhea) are impaired.
Types of relapse
After tumor removal, the risk of:
- early relapses (less than 2 years);
- intermediate relapses (from 2 to 5 years);
- distant relapses (later than five years).
More often, the disease returns in the first two years (about 65% of cases). Based on the location of recurrent cancer, tumors of the following locations are distinguished:
- zones of interintestinal connection;
- mesentery;
- peritoneum;
- retroperitoneal space.
According to foreign authors, in patients with stage I of the process, relapses occur from 0 to 13%, in patients with stage II - from 11 to 60%, in patients with stage III - from 32 to 88%.
Postcholecystectomy syndrome. Diagnostics
Diagnostics is aimed at identifying various diseases of the gastrointestinal tract that the patient had before surgery, those that arose after surgery, and possible postoperative complications.
The diagnosis is made based on:
- clinical manifestations of the disease (patient complaints),
- objective data from the examination of the patient,
- laboratory data (biochemical blood test, clinical blood test, indicators of metabolic processes - lipid, carbohydrate metabolism, enzymatic function of the pancreas, intestinal microflora),
- instrumental examination methods (X-ray, ultrasound, gastroduodenoscopy),
- in more severe cases - endoscopic retrograde cholangiography, computed tomography, dynamic scintigraphy.
Diagnostics
The oncologist begins to identify a relapse at the time of interviewing and examining the patient. A stool test for the presence of blood is used as a screening test. If rectal cancer occurs, the diagnosis can be confirmed using a rectal examination. If a relapse of the overlying parts of the intestine is suspected, an endoscopic diagnostic method is used - sigmoidoscopy or colonoscopy.
During the examination, the doctor can visually assess the presence of a lesion(s), its size, prevalence and growth pattern. Material must be taken for histological confirmation of relapse.
To search for distant metastases, ultrasound or CT of the abdominal organs, radiography of the spine, CT of the lungs, MRI of the brain and other methods are prescribed. Sonography is performed to confirm the presence of cancer in the lymph nodes.
Postcholecystectomy syndrome. Treatment and prevention
In the early postoperative period, therapeutic nutrition is of great importance, which often involves split meals up to 6 times a day, in small portions with fat limited to 60-70 g per day.
In order to more quickly adapt the digestive system to new physiological conditions - functioning without a gallbladder, taking into account concomitant diseases, an earlier expansion of nutrition close to rational is recommended.
Postcholecystectomy syndrome. Drug therapy according to indications
In order to improve the quality of bile produced by the liver, ursodeoxycholic acid preparations (Ursosan, Ursofalk, Ursodez, Livodexa, Exchol, Choludexan, Ursodoxa, etc.) are prescribed. The dose and duration of taking the drug is determined by the attending physician.
To bind excess bile into the intestines and especially the presence of chologenic diarrhea, sorbents (Smecta) and antacids (Phosphalugel, Maalox, Alyagel, etc.) are prescribed, 1 package 3-4 times a day 1 hour after meals for 7-14 days, regimen reception and duration are determined individually.
If there is pain in the upper abdomen, antispasmodics are prescribed (for example, Duspatalin 1 capsule 2 times a day, Dicetel 50-100 mg 3 times a day for 2-4 weeks).
In the presence of duodenitis, papillitis, or the appearance of opportunistic flora in stool cultures, a 7-day course of antibacterial drugs is administered. The drugs of choice may be Ercefuril, Intetrix, Furazolidone, etc., less often antibiotics in standard doses.
In the presence of concomitant pathology (pancreatitis, etc.), enzyme preparations (Pancreatin, Mezim forte, Creon, etc.) are prescribed according to indications.
Postcholecystectomy syndrome. Prevention
Prevention of PHES begins already in the process of preparation for surgery in order to identify and timely treat diseases of the hepatopancreatoduodenal zone (liver diseases, pancreatitis, duodenitis and erosive-ulcerative process in the duodenum).
The doctor is especially concerned about the condition of the pancreas, and if chronic pancreatitis is detected before surgery, it is necessary to carry out a course of treatment (antisecretory drugs, antispasmodics, enzyme preparations, ursodeoxycholic acid preparations). These measures reduce the risk of exacerbations of pancreatitis in the postoperative period by 2.5-3 times.
Rehabilitation
Experience shows that signs of postcholecytectomy syndrome more often occur in the first year of observation during the period of adaptation of the digestive tract to new anatomical conditions.
After 3-6 months, although there is currently information about the successful use of low-salinity mineral waters after the 10th day after surgery, the intake of mineral waters is indicated, optimally in the conditions of a gastroenterological drinking resort (Zheleznovodsk, Kashin, Dorokhovo, Karlovy Vary, etc.) with repeating the course of mineral water at home after six months.
Clinical follow-up of patients is carried out during the first year after surgery.
Features of the postoperative course of patients after gastrectomy and gastrectomy
A gastrectomy operation is the complete removal of the stomach with both omentums and regional lymph nodes, ending with a direct connection of the esophagus to the jejunum. This is a serious injury to the body, but the patient must understand that it is due to the tasks of preserving his life, and therefore it is necessary to assess the consequences of the operation and prepare for the correct adaptation of the body to the new conditions of food processing.
A frequent complication of this operation is reflux esophagitis - reflux of the contents of the jejunum into the esophagus, irritation of the latter by pancreatic juice and bile.
Reflux syndrome occurs more often after eating fatty foods, milk, fruits and is expressed in a feeling of acute pain and burning behind the sternum and in the epigastric region. Taking a hydrochloric acid solution neutralizes alkaline pancreatic juice and soothes pain. If reflux syndrome persists for a long time and debilitates the patient, X-ray or endoscopic examination is recommended to exclude a possible relapse of the disease. Much more often than after gastrectomy, gastrectomy is complicated by dumping syndrome (see below).
Anemic syndrome after gastrectomy is expressed in increasing anemia (anemia) with concomitant dyspeptic disorders. It is a consequence of the absence of Castle factor, produced by the gastric mucosa.
After total gastrectomy, general disorders also occur: poor health, asthenia, progressive weight loss.
Prevention of these complications is possible . It consists of strict adherence to the diet and diet prescribed to the patient. Those who have undergone a total gastrectomy (1.5-3 months after surgery) - a hyposodium, physiologically complete diet with a high protein content, limitation of fats and complex carbohydrates to the lower limit of normal and a sharp limitation of easily digestible carbohydrates, with a moderate limitation of mechanical and chemical irritants of the mucous membrane and the receptor apparatus of the gastrointestinal tract. Exclude stimulants of bile secretion and pancreatic secretion. All dishes are prepared boiled or steamed (see section “therapeutic nutrition”). Eating 5-6 times a day in small portions, thoroughly chewing food taken with weak solutions of hydrochloric or citric acids.
Systematic monitoring of the patient’s nutrition is carried out according to the height-weight indicator (HWI) - (body weight in kg ×100÷height in cm). The value of RVP in the range of 33-38 indicates a satisfactory nature of nutrition, below 33 - low, and above 38 - good nutrition of the patient. The energy value of the products is 2500-2900 kcal/day.
Some patients, on the contrary, cannot withstand long-term adherence to the diet, violate it, switch to 3-4 meals a day, and systematically do not take gastric juice or hydrochloric acid solutions. As a result, intestinal function is impaired and anemia progresses.
Complete physiological rehabilitation of patients occurs at a later date - by the end of the first year after surgery. Psychosocial rehabilitation in some patients is hampered by suspiciousness. Before the operation, they were worried about the question: how much will be cut out? After surgery - how to live without a stomach? As a result of suspiciousness, they excessively restrict nutrition. Lack of protein and plant foods leads to exhaustion and vitamin deficiency.
Important! It must be remembered that all patients with gastroenterological problems, without exception, have psychological problems - suspiciousness, phantom pain, anxiety and depression, “withdrawal into illness” and the search for symptoms that are not related to the disease. In such patients, psychosomatic pathology arises, complicated by the treatment and the diagnosis itself.
The people around him are called upon to help the patient prevent these complications. It is necessary to maintain strict medical discipline. Changes in diet should not be allowed. The method of influencing the patient is a friendly conversation with the patient about the need to strictly follow the doctor’s recommendations.
Another surgical option. During gastric resection, not the entire stomach, but most of the stomach (3/4 or 4/5) with both omentums and regional lymph nodes are removed along with the tumor. The stump of the stomach is usually connected to the jejunum. As a result of the operation, the body is deprived of the main zones of the motor and secretory functions of the stomach and its outlet section, which regulates the flow of food from the stomach into the intestines as it is processed. New anatomical and physiological conditions for digestion are being created, leading to a number of pathological conditions associated with surgery and being its consequences.
Painful symptoms appear, called dumping syndrome (reset syndrome). Insufficiently processed food from the stomach goes directly into the jejunum in large portions. This causes irritation of the initial part of the jejunum. Immediately after or during a meal, a feeling of heat, palpitations, sweating, dizziness to the point of fainting, and severe general weakness occur. These phenomena gradually disappear soon (15-20 minutes) after assuming a horizontal position. In other cases, nausea, vomiting and spastic pain occur within 10-30 minutes. after meals and last up to 2 hours. They are the result of rapid movement of food through the jejunal loop and exclusion of the duodenum from digestion. Dumping syndrome does not pose an immediate threat to life, but it frightens patients and darkens their existence if the necessary preventive measures are not taken. The diet should contain fewer carbohydrates (potatoes, sweets) and more protein and fatty foods. Sometimes they are prescribed 10-15 minutes in advance. before meals, 1-2 tablespoons of 2% novocaine solution.
Insufficient motor function of the stomach can be compensated for by thoroughly chewing food and eating slowly; The secretory function of the stomach can be regulated by taking gastric juice or solutions of hydrochloric and citric acids during meals. In the absence of the pyloric stomach, it is necessary to prescribe split meals with meals 5-6 times a day.
Upon discharge from the hospital, the patient and relatives receive detailed instructions about diet and nutrition. They should not be forgotten. A hyposodium (salt restriction), physiologically complete diet with a high protein content, a normal content of complex carbohydrates and a sharp limitation of easily digestible carbohydrates, and a normal fat content is recommended.
It should contain limited content of mechanical and chemical irritants of the mucous membrane and the receptor apparatus of the gastrointestinal tract (pickles, marinades, smoked foods, canned food, hot, cold and carbonated drinks, alcohol, chocolate, spices, etc.), the content of nitrogenous extractives (especially purines), refractory fats, aldehydes, acroleins.
Avoid strong stimulants of bile secretion and pancreatic secretion, as well as foods and dishes that can cause dumping syndrome (sweet liquid milk porridges, sweet milk, sweet tea, hot fatty soup, etc.). All dishes are prepared boiled or steamed, pureed. In case of severe clinical symptoms, it is better to use ready-made clinical nutrition products specially produced for cancer patients. Energy value – 2800-3000 kcal/day. The patient should pay special attention to the importance of eating food slowly, chewing it thoroughly, and the systematic and mandatory intake of hydrochloric acid solutions.
To protect tooth enamel from the destructive effect of hydrochloric acid on it, patients are usually recommended to prepare for themselves weak solutions of it in fruit juice or fruit drink. For 1 liter of fruit juice - 1 tablespoon of a 3% solution of hydrochloric (hydrochloric) acid. Take this acidified fruit drink in sips during meals. It is harmless to teeth and pleasant. If you follow the diet, diet, and systematic intake of hydrochloric acid solution, complete rehabilitation of the patient with restoration of ability to work occurs in the next 4-6 months.
If symptoms of gastric pathology occur a long time after surgery, a recurrence of the malignant tumor can be assumed. The light interval from the moment of radical surgery to the appearance of signs of cancer recurrence in the gastric stump usually lasts 2-3 years; for relapse after total gastrectomy (in the area of anastomosis with the esophagus) – one year.
Aching pain in the epigastric region associated with the intake and nature of food, belching, vomiting are indications for referring the patient for an emergency examination by an oncologist, examining him X-ray and endoscopically. This is also necessary in cases where the light gap is significantly smaller.
Read about stomach cancer on the website www.gastriccancer.ru
SIGN UP FOR A CONSULTATION by phone +7 (812) 951 - 7 - 951





![Table 4. Major muscular dystrophies accompanied by increased CPK levels [41]](https://ddpskov.ru/wp-content/uploads/tablica-4-osnovnye-myshechnye-distrofii-soprovozhdayushchiesya-povysheniem-urovnya-kfk-41-330x140.jpg)



