Studying the structure of the human body is a difficult but interesting activity, because studying your own body helps you to know yourself, others and understand them.
A person cannot help but breathe. After a few seconds, his breathing repeats, then after a few more, again, again, and so on for the rest of his life. The respiratory organs are important for human life. Everyone needs to know where the bronchi and lungs are located in order to understand their feelings during the period of illness of the respiratory system.
Lungs: anatomical features
The structure of the lungs is quite simple; for each person they are approximately the same normally, only the size and shape may differ. If a person has an elongated chest, the lungs will also be elongated and vice versa.
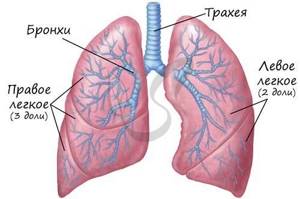
This organ of the respiratory system is vital, as it is responsible for providing the entire body with oxygen and removing carbon dioxide. The lungs are a paired organ, but they are not symmetrical. Every person has one lung larger than the other. The right one is large in size and has 3 lobes, while the left one has only 2 lobes and is smaller in size. This is due to the location of the heart on the left side of the chest.
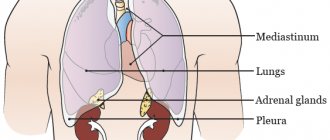
Lung location
The lungs are located in the middle of the chest. They are protected and supported by a frame of ribs, 12 on the left and right. On the back side, the organs are protected by the spinal column.
To ensure the ability to breathe, there is muscle tissue between the ribs; the bones are fixed to the sternum by cartilage. From the back, the lungs are located 2-3 cm above the collarbones.
From below, the organ borders the diaphragm, which separates the peritoneum and chest. On the right side, under the lung, is the liver. On the left side, the heart is adjacent on top, and partly the stomach is below. The exact location of a person’s lungs can be clearly seen in the photo.
Structural elements of the lungs
This organ has only 3 important elements, without which the organ will not be able to perform its functions.
- Bronchi.
- Bronchioles.
- Alveoli.
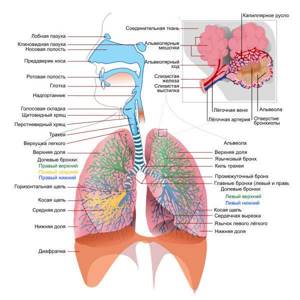
To know where the bronchi are located in the body, you need to understand that they are an integral part of the lungs, therefore the bronchial tree is located in the same place as the lungs, in the middle of this organ.
Bronchi
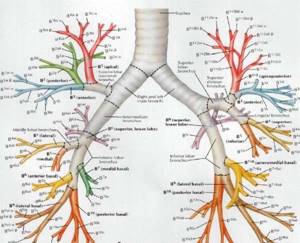
The structure of the bronchi allows us to talk about them as a tree with branches. They look like an overgrown tree with small branches at the end of the crown. They continue the trachea, dividing into two main tubes, in diameter these are the widest passages of the bronchial tree for air.
When the bronchi branch, where are the small air passages located? Gradually, as they enter the lungs, the bronchi divide into 5 branches. The right section of the organ is divided into 3 branches, the left into 2. This corresponds to the lobes of the lungs. Then more branches occur, during which a decrease in the diameter of the bronchi occurs, the bronchi are divided into segmental ones, and then even smaller. This can be seen in the photo with the bronchi. There are 18 such segments in total, 8 on the left side and 10 on the right.
The walls of the bronchial tree consist of closed rings at its base. Inside, the walls of the human bronchi are covered with mucous membrane. When infection penetrates into the bronchi, the mucous membrane thickens and narrows in diameter. Such an inflammatory process can reach the human lungs.
Bronchioles
These air passages are formed at the ends of branched bronchi. The smallest bronchi, located separately in the lobes of the lung tissue, have a diameter of only 1 mm. Bronchioles are:
- end;
- respiratory.
This division depends on where the branch with the bronchioles is located in relation to the edges of the tree. At the ends of the bronchioles there is also their continuation - the acini.
The acini may also look like branches, but these branches are already independent and have alveoli on them - the smallest elements of the bronchial tree.
Alveoli
These elements are considered microscopic pulmonary vesicles, which directly perform the main function of the lungs - gas exchange. There are a lot of them in the lung tissue, so they cover a large area for the delivery of oxygen to a person.
The alveoli in the lungs and bronchi have very thin walls. When a person simply breathes, oxygen penetrates through these walls into the blood vessels. In the blood stream it is found by red blood cells, and with red blood cells it travels to all organs.
People don’t even think about the fact that if these alveoli were a little smaller, there would not be enough oxygen for the functioning of all organs. Due to their tiny size (0.3 mm in diameter), the alveoli cover an area of 80 square meters. Many people don’t even have housing with such space, but their lungs can accommodate it.
Lungs
Lung structure
The lungs are paired organs located in the chest cavity. They consist of lobes: the right lung contains three lobes, the left - two. Lung tissue consists of bubbles - alveoli, in which a vital process occurs - gas exchange between blood and atmospheric air.
The lung is covered with a membrane - the pleura, which passes from the surface of the lungs to the inner walls of the chest. A pleural cavity is formed between the two layers of the pleura, the pressure in which is lower than atmospheric (it is called negative pressure), which is of fundamental importance for the act of inhalation and exhalation.
Gas exchange in the lungs and tissues
The air moves along the airways and finally reaches the smallest structure of the lung - the pulmonary vesicle, or alveoli. The wall of the alveoli is intertwined with a dense network of capillaries - vessels with a thin wall through which gases diffuse: carbon dioxide leaves the blood into the alveoli, and oxygen enters the blood from the alveoli.
Oxygen dissolved in the blood reaches the internal organs and tissues of the body through the blood vessels. I note that moving through the blood, gases form compounds with hemoglobin in red blood cells:
- Oxygen (O2) - oxyhemoglobin
- Carbon dioxide (CO2) - carbhemoglobin
- Carbon monoxide (CO) - carboxyhemoglobin
The combination of hemoglobin with carbon monoxide is much more stable than the others: carbon monoxide easily wins the competition with oxygen and takes its place. This explains the severe consequences of carbon monoxide poisoning, which quickly accumulates during a fire in a confined space.
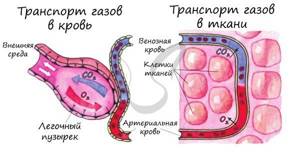
As the blood gives up carbon dioxide and takes in oxygen, it turns from venous blood (poor in oxygen) into arterial blood. In tissues, the reverse process occurs: cells need oxygen necessary for tissue respiration, and carbon dioxide, a byproduct of metabolism, requires removal from the cell into the blood.
I often ask students, “What moves the gas, what causes, for example, oxygen to move first from the alveoli to the blood, and in the tissues from the blood to the cells?” Remember that this driving force is the difference in partial pressure of gases.

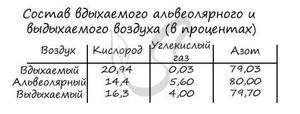
The partial pressure of a gas is that part of the total volume of gas that falls on the share of this gas. I do not recommend that you memorize the table above, but it is quite good for understanding.
Note that the partial pressure of oxygen in the alveoli is 100-110, and in the venous blood of the capillary that encircles the wall of the alveoli, the oxygen pressure is 40. Thus, oxygen rushes from an area of higher pressure to an area of lower pressure - from the alveoli into the blood.
The ongoing movements of gases can be easily recorded by measuring the concentration of gases in the air inhaled and exhaled by a person. You probably won't need much of this information, but I encourage you to remember that the ambient air contains 21% oxygen and 0.03% carbon dioxide - this is important information.
The liquid covering the walls of the alveoli - surfactant - is important in the transport of gases. Initially, oxygen dissolves in the surfactant and only then diffuses through the capillary wall, entering the blood. Surfactant also prevents the walls of the alveoli from sticking together (collapsing) during exhalation.
Vital capacity of the lungs
One of the physiologically important indicators is vital capacity (VC). Vital capacity is the maximum amount of air that a person can exhale after the deepest breath.
This indicator is very variable; the average vital capacity of an adult is about 3500 cm3. In athletes, vital capacity is 1000-1500 cm3 more, and in swimmers it can reach 6500 cm3. The greater the vital capacity, the more air enters the lungs and oxygen enters the circulatory system, which is very important for tissue cells during sports.
Vital vital capacity is easily measured using a special device - a spirometer (from the Latin spirare - to breathe).

Mechanism of pulmonary respiration
Between the outer surface of the lung and the walls of the chest there is a pleural cavity, which plays a vital role in the process of inhalation and exhalation, and also reduces friction of the lungs during breathing movements.
The pressure in the pleural cavity is always 5-7 mm lower. rt. Art. atmospheric pressure, so the lungs are constantly in an expanded state, fastened through the pleura to the walls of the chest cavity.

Imagine: the lung is pulled up to the pleura, which is attached to the chest. And the chest constantly makes breathing movements, expanding and contracting, thus the lung follows the respiratory movements of the chest.
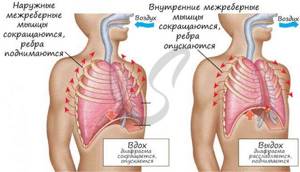
It remains to figure out how these respiratory movements occur? The reason for this is the contraction and relaxation of the intercostal muscles, as a result of which the chest rises and falls, respectively. Now we will discuss in detail the mechanism of inhalation and exhalation.
When inhaling, the external intercostal muscles contract, while the ribs rise, and the sternum moves forward - the chest expands in the anteroposterior and frontal (to the sides) directions. The diaphragm is a respiratory muscle; during inhalation it contracts and moves down: the chest expands in the vertical direction.
When you exhale, the internal intercostal muscles contract, the ribs lower, the sternum moves back - the chest narrows in the anteroposterior and frontal (to the sides) directions. During exhalation, the diaphragm relaxes and rises: the chest narrows in the vertical direction. Thanks to these movements, inhalation and exhalation are carried out.
Can we take control of our breathing? Easily. But we don’t always control it even during the day, let alone at night. The breathing process is controlled by the respiratory center located in the medulla oblongata of the brain. The respiratory center is automatic - periodically impulses themselves flow to the respiratory muscles, for example, during sleep.
The composition of the blood greatly affects the intensity of breathing. Numerous experiments have shown that an increase in CO2 concentration stimulates the respiratory center. This can explain the increase in breathing during physical activity, for example, running, when CO2 is actively formed in the muscle cells of the legs and enters the blood, breathing becomes more frequent reflexively.
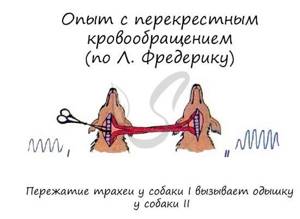
The reflex regulation of breathing is most clearly demonstrated by the experiment with cross circulation, in which the circulatory systems of two dogs are connected. When the trachea is compressed, the first dog stops breathing, and carbon dioxide stops being removed from the blood - its concentration in the blood increases, which leads to shortness of breath (rapid breathing) in the second dog.
Pneumothorax
Normally, the pressure in the pleural cavity is negative, which stretches the lungs. However, with injuries to the chest, the integrity of the pleural cavity may be disrupted: in this case, the pressure in the cavity becomes equal to atmospheric pressure.
Violation of the integrity of the pleural cavity is called pneumothorax (from the ancient Greek πνεῦμα - blow, air and θώραξ - chest). When pneumothorax occurs, the lungs collapse and cease to participate in breathing.

Mountain and decompression sickness
Climbers and mountain hikers (especially beginners) often experience altitude sickness. This condition occurs due to the fact that when rising to a height, the partial pressure of oxygen drops, and its concentration in the blood does not meet the body's needs - it is lower than it should be.
At first, mountain sickness manifests itself as euphoria (unreasonable joy) and increased heart rate. If the conquest of mountain peaks continues, then these symptoms are gradually joined by apathy (a state of indifference), muscle weakness, cramps and headache.
What to do, you ask? It is necessary to immediately stop further ascent, and if symptoms worsen, begin descent. It is best to prevent altitude sickness by following the rule - do not increase the altitude of your overnight stay by more than 300-600 meters.

Caisson disease occurs in divers and is associated with an increase in the partial pressure of a gas - nitrogen, which occurs when diving under water. There is a pattern: the deeper the diver descends, the more nitrogen becomes dissolved in the blood. What is the danger of nitrogen dissolving in the blood?
With a sharp, rapid rise, the solubility of nitrogen in the blood decreases, and the blood literally boils. Just imagine, real gas bubbles appear in the vessels! They can clog the vessels of the lungs, heart, and other internal organs, as a result of which blood circulation stops, and the consequences can be very sad, even fatal.
How to prevent decompression sickness? You can use helium gas in the breathing mixture instead of nitrogen, which does not lead to such consequences. It is also necessary to adhere to the rule of gradual ascent, with stops, and avoid sudden ascent.

© Bellevich Yuri Sergeevich 2018-2021
This article was written by Yuri Sergeevich Bellevich and is his intellectual property. Copying, distribution (including by copying to other sites and resources on the Internet) or any other use of information and objects without the prior consent of the copyright holder is punishable by law. To obtain article materials and permission to use them, please contact Yuri Bellevich
.
Volume of the main organ of the respiratory system
Located in the middle of the human body, near the heart, the lungs perform a number of important functions. We already know that they supply oxygen to all organs and tissues. In full, this happens simultaneously, but this organ also has the ability to store oxygen due to the alveoli located in it.
The lung capacity is 5000 ml - this is what they are designed for. When a person inhales, he does not use the full volume of his lungs. Typically, 400-500 ml are required for inhalation and exhalation. If a person wants to take a deep breath, he uses approximately 2000 ml of air. After such inhalation and exhalation, a reserve of volume remains, which is called functional residual capacity. It is thanks to it that the required level of oxygen is constantly maintained in the alveoli.
Blood supply
Two types of blood circulate in the lungs: venous and arterial. This respiratory organ is very closely surrounded by blood vessels of different sizes. The most basic is the pulmonary artery, which then gradually divides into small vessels. At the end of the branching, capillaries are formed that entwine the alveoli. Very close contact and allows for gas exchange in the lungs. Arterial blood nourishes not only the lungs, but also the bronchi.
This main respiratory organ contains not only blood vessels, but also lymphatic vessels. In addition to the various branches, nerve cells also branch in this organ. They are very closely interconnected with blood vessels and bronchi. Nerves can create vascular-bronchial bundles in the bronchi and lungs. Because of this close relationship, doctors sometimes diagnose bronchospasm or pneumonia due to stress or another malfunction of the nervous system.
Surgical method for treating lung cancer
- the main radical method for stages 1-3 of the disease. Operations performed for this disease are classified:
- by volume of resection (lobectomy (removal of a lobe of the lung), bilobectomy (removal of two lobes of the lung), pneumonectomy (removal of the entire lung)),
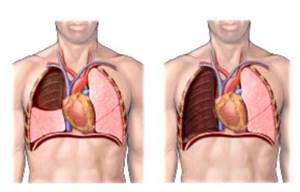
Photo 3 - Lobectomy
Photo 4 - Pneumonectomy
- by volume of removal of lymph nodes of the thoracic cavity (standard, expanded, super-expanded),
- by the presence of resection of adjacent organs and structures (combined operations are performed when the tumor grows into the pericardium, trachea, superior vena cava, esophagus, aorta, atrium, chest wall, spine). In addition to surgical treatment, it is possible to use an integrated approach, including radiation and chemotherapy.

When treating locally advanced malignant tumors with transition to the main bronchus and pulmonary artery, in cases where previously the only option for surgical treatment was pneumonectomy, it is now possible to perform organ-preserving operations. In this case, the affected area of the main bronchus is excised, followed by restoration of continuity (bronchoplastic and angioplastic lobectomies)
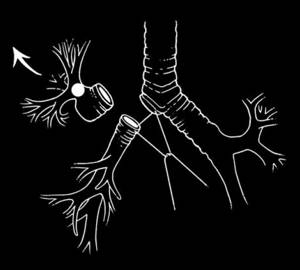
Photo 5 - Scheme of upper bronchoplastic lobectomy
Additional functions of the respiratory organ
In addition to the well-known function of exchanging carbon dioxide for oxygen, the lungs also have additional functions due to their structure and structure.
- Affect the acidic environment in the body.
- They cushion the heart - in case of injury, they protect it from shocks and various influences.
- They secrete the substance immunoglobulin A, compounds against bacteria that protect the human body from infections of viral etiology.
- They have a phagocytic function - they protect the body from the penetration of a large number of pathogenic cells.
- They provide air for conversation.
- They take part in preserving a small amount of blood for the body.
Formation of the respiratory organ
The lungs are formed in the thorax of the embryo as early as 3 weeks of pregnancy. Already from the 4th week, bronchopulmonary kidneys gradually begin to form, from which 2 different organs are then formed. Closer to the 5th month, bronchioles and alveoli form. By the time of birth, the lungs and bronchi are already formed and have the required number of segments.
After birth, these organs continue to grow, and only by the age of 25 does the process of the appearance of new alveoli end. This is due to the constant need for oxygen for a growing organism.
Life forecast
The prognosis of lung cancer in NSCLC includes symptoms, tumor size (> 3 cm), non-squamous histology, extent of spread (stage), lymph node metastasis and vascular invasion. Inoperability of the disease, severe symptoms and weight loss of more than 10% give lower results. Prognostic factors for small cell lung cancer include condition status, sex, stage of disease, and involvement of the central nervous system or liver at the time of diagnosis.
For non-small cell lung cancer, the prognosis for life with complete surgical resection of stage IA (early stage of the disease) is 70% five-year survival.





![Table 4. Major muscular dystrophies accompanied by increased CPK levels [41]](https://ddpskov.ru/wp-content/uploads/tablica-4-osnovnye-myshechnye-distrofii-soprovozhdayushchiesya-povysheniem-urovnya-kfk-41-330x140.jpg)

