Computed tomography of the throat is one of the new ways to examine bone structures and soft tissues in this area. Diagnostics provides an opportunity to identify existing pathological conditions and structural features of the tissues of the larynx. Through scanning, you can obtain highly accurate images of the part of the body being examined, and therefore making the correct diagnosis will not cause difficulties for a specialist.
What you need to know about throat cancer
- A small percentage is adenoid cystic cancer.
- Most cases of pharyngeal cancer are squamous cell carcinoma.
- Incidence: 10-35%
- Mostly men are affected.
Nasopharynx: Increased incidence among Chinese (18%)
- Accounts for 70-95% of all tumors of the nasopharynx, oropharynx and hypopharynx.
Oropharynx and hypopharynx: Increased incidence with alcohol abuse and smoking
- The incidence, spread, and lymph node involvement depend on the location of the tumor.
Nasopharynx: Schminke tumor
- Develops when exposed to carcinogens and the Epstein-Barr virus
- In 90% of cases, lymph node involvement is present at the time of diagnosis
- There are three subtypes:
— Type 1: Keratinizing.
— Type 2: Non-keratinizing.
— Type 3: Undifferentiated.
Oropharynx: 80% - tonsils
- 15% - soft palate
- 4% - pharynx
- In 60% of cases, lymph node involvement is present at the time of diagnosis.
Laryngopharynx:
- Tumor ulceration or exophytic growth is often observed
- 60% - pyriform sinus
- 25% - posterior to the cricoid cartilage of the larynx
- 15% - posterior pharyngeal wall
- In 50% of cases, lymph node involvement is observed at the time of diagnosis.
Alternative diagnostic methods
Alternative diagnostic methods include ultrasound and magnetic resonance imaging. However, CT of the throat has a clear advantage - this method is the most informative and fastest. In addition, it allows you to identify even minor pathological processes and evaluate the structures of internal organs.
If we talk about which type of diagnosis is better: MRI or CT, then it will be quite difficult to answer this question unambiguously. Both research methods serve completely different purposes, although many of the data obtained may be duplicated.
A CT scan of the throat is performed using X-rays, so it allows you to examine dense formations and hollow organs. Magnetic resonance imaging is the best way to identify soft tissue conditions and is widely used to evaluate injuries to the neck and ligaments.
If there is a need to scan patients in an emergency situation, the choice of one or more examination methods is at the discretion of the doctors, based on the nature of the pathological condition.
Clinical manifestations
Typical symptoms:
- Pharyngeal cancer often has nonspecific symptoms, such as a painless, non-healing ulcer of the pharyngeal mucosa
- Speech Impairment
- Dysphagia
- Neurological disorders - only at stage T4
- Often, lymph node involvement is already present at the time of diagnosis.
— Metastasis of nasopharyngeal cancer (in descending order of frequency): Lymph nodes, bones, lungs, liver.
— Metastasis of oropharyngeal cancer (in descending order of frequency): Lymph nodes, lungs, bones, liver.
Structure of the human throat
The throat is an important and very complex system of the human body that performs several basic functions. It is through the throat that the esophagus passes; it is this part of the respiratory system that provides a person with the ability to swallow, talk and, in general, breathe. The throat starts from the nasal cavity and mouth and runs all the way to the trachea.
The system includes two main components - the larynx (larynx), which ensures the functioning of the vocal cords and the pharynx (pharynx), which facilitates the swallowing of food and its entry into the stomach, and it also provides air supply to the lungs.
The structure of the throat in children and adults is almost identical, except that in children all components of the respiratory system are smaller in diameter. And if various inflammatory processes occur in this area, this can cause swelling in an adult, while in a child it can block breathing.
Signs of pharyngeal cancer on MRI and CT scans of the neck
Selection Methods
- MRI
- CT
What will CT scans of the throat show for cancer?
- Massive formation with invasive growth located next to the pharyngeal mucosa
- Often defined as an asymmetric lesion with unclear contours and moderate enhancement after administration of contrast agent.
In what cases is an MRI needed for throat cancer?
- The tumor is hypo- or isointense to muscle on T1-weighted images, making it clearly demarcated from fat tissue
- Slightly hyperintense on T2-weighted image, in which case fat suppression helps to define tumor boundaries
- Minimal enhancement after gadolinium administration
- Tumor boundaries are better visible when using a fat-suppressed sequence
- Attention: The tumor can infiltrate the membranes of the neurovascular bundles, bones and muscles.
Features
- Often an inhomogeneous pharyngeal mass, which can infiltrate adjacent structures depending on the stage of the tumor.
Pharyngeal cancer classification (AJCC):
- Nasopharynx:
- T1 (limited to one anatomical region, submucosal tumor only)
- T2 (affects multiple anatomical sites)
- TZ (applies to the nasal cavity, oropharynx)
- T4 (extends to base of skull, cranial nerves).
- Oropharynx:
- Tis (cancer in situ)
- T1 (<2 cm)
- T2 (2-4 cm)
- TZ (>4 cm)
- T4 (invasive growth).
— Laryngopharynx:
- T1 (limited to one anatomical region, <2 cm)
- T2 (affects several anatomical areas or 2-4 cm without fixation of the larynx)
- TZ (more than 4 cm or presence of laryngeal fixation)
- T4 (invasion of adjacent structures).
What does a CT scan of the larynx reveal?
Using CT images, specialists have the opportunity to visualize a number of diseases and pathological conditions:
- neoplasms of soft and bone tissues of the larynx with the ability to assess their size and location;
- presence of esophageal diverticula;
- places of destruction of cartilage in the larynx;
- observe changes in the structure of the walls of the larynx, which may be a sign of a developing tumor;
- identify the presence of foreign bodies in the area being examined;
- determine the severity of injuries received;
- assess the condition of the lymph nodes;
- identify existing inflammatory processes in the cavity being examined;
- diagnose various developmental pathologies;
- examine the vascular network of the larynx.
What pathologies are there symptoms of pharyngeal cancer?
Tonsil hyperplasia (nasopharynx or oropharynx)
-Usually symmetrical, homogeneous enlargement of the tonsils on both sides
— No invasive growth
— Strengthening partitions
— Most patients are under 20 years of age
Damage to the tonsils in non-Hodgkin's lymphoma (nasopharynx or oropharynx)
— Unilateral tumor formation spreading in the submucosal layer
— Marked enlargement of lymph nodes without signs of necrosis
Benign tumors of the salivary glands (eg, adenoma) (nasopharynx or oropharynx)
— Non-invasive tumor with smooth edges
- The tumor may be pedunculated and cause a narrowing of the pharynx
— No reinforcement of partitions
Malignant tumors of the salivary glands (eg, cancer) (nasopharynx, oropharynx, or hypopharynx)
— Adenocystic carcinoma, the morphological picture resembles squamous cell carcinoma
- Often difficult to distinguish from squamous cell carcinoma
— Lymph node metastases are rare or absent
Kaposi's sarcoma (hypopharynx)
- AIDS-associated tumor
— Mucosal lesions similar to squamous cell carcinoma
Abscess
Acute clinical symptoms
— Abscess capsule
Progress of CT scan of the larynx
To conduct a CT scan of the throat and larynx, the patient is asked to take a horizontal position on a sliding table, where he will remain for the duration of the study.
His body is fastened with belts for secure fixation, after which the table slides inside the device. All that is required of the patient during a CT scan of the throat is to remain completely calm and not make any movements. The tomograph scans, resulting in a series of images. As a rule, the entire examination process takes no more than 15-20 minutes.
During the scan, the patient is alone in the room. Medical staff monitors the examination progress through a special window from an adjacent office. The patient is not left for a minute without the supervision of doctors. Both the patient and the doctors have the opportunity to communicate through the use of a microphone, so if there are any changes in well-being, the patient will always be able to inform the staff and not be afraid that he is isolated from the outside world.
The latest generation of tomographs meets all safety requirements, so they do not pose any significant harm to the health of patients. Although CT is based on X-ray radiation, it has a very low intensity and, when compared with a classic X-ray examination, it is quite insignificant.
However, due to the fact that X-rays are used during a CT scan of the larynx, this procedure cannot be called absolutely harmless, and it has certain time restrictions for repeated scanning.
Thus, it is unacceptable for women who are expecting the birth of a baby to undergo a CT scan, regardless of the stage of pregnancy, as well as for patients who have already undergone this type of examination in the recent past.
A CT scan of the throat cannot be performed an unlimited number of times, since the radiation dose cannot be exceeded. And only in exceptional cases, if there is strong evidence for this, specialists can prescribe an additional CT examination.
Possible complications and consequences
Pharynx cancer has complications such as:
- Hoarseness to aphonia
- Pharyngeal stenosis
- Bleeding during surgery and in the postoperative period
CT with contrast: cancer of the hypopharynx. In the pyriform recess, a tumor formation is observed with moderate enhancement in the posterolateral regions, which causes asymmetric narrowing of the pharynx. The tumor crosses the midline and extends to the peripharyngeal space on the left.
CT scan with contrast: nasopharyngeal cancer (Schminke tumor). There is bone infiltration and focal invasion into the base of the skull with intracranial extension along the clivus. The tumor tissue grows into the carotid canal (infiltration of the internal carotid artery is possible). Lipomatosis of the tongue muscles is determined due to tumor invasion of the hypoglossal nerve.
Contraindications for diagnostics
CT scan of the throat and larynx has some contraindications for the following patients:
- women expecting the birth of a baby;
- patients with excess body weight;
- patients with mental illness.
CT scans are performed with extreme caution:
- children under 12 years of age;
- women breastfeeding babies;
- patients with kidney problems;
- patients with multiple myeloma.
Carrying out computed tomography using contrast is unacceptable:
- during pregnancy and breastfeeding;
- patients with disorders of the liver and kidneys;
- diabetics;
- patients with an allergic reaction to contrast.
Treatment of laryngeal cancer
Laryngeal cancer can form in any part of the larynx, and the treatment methods that can be applied in a particular case of the disease depend on this. Treatment tactics are determined based on the stage of the disease and other factors that determine the patient’s general health.
For tumors diagnosed in the early stages, it is possible to use the most modern method of gentle treatment, without surgical removal of the larynx - remote radiosurgery using the CyberKnife . In advanced stages of the disease, combination treatment is used, which may include surgery, radiation therapy and chemotherapy.
A patient's story about treatment for a type of laryngeal cancer.
The sequence of treatment methods may differ for different cases of the disease; the decision on tactics to combat the disease is made by doctors at an interdisciplinary council.
Surgery
In most cases, surgical treatment of laryngeal cancer involves the use of minimally invasive surgical techniques. This helps to reduce the time of the operation itself and speed up the patient’s recovery after surgery.
Surgeries for laryngeal cancer may include complete or partial removal of the organ with adjacent lymph nodes. The extent of surgical intervention depends on the extent of the malignant tumor and the stage of the cancer.
Radiation therapy

Radiation therapy IMRT for laryngeal cancer
Radiation therapy plays an important role in the combined treatment of the disease. The most modern method of radiation treatment of tumors is used - high-precision intensity modulated radiation therapy (IMRT).
IMRT technology allows you to create zones of high dose of ionizing radiation, incl. complex spatial shapes that exactly match the shape and size of the tumor. This allows the delivery of high doses of ionizing radiation into the volume of a malignant tumor, which leads to the death of cancer cells. At the same time, the surrounding tissues and organs within the tumor remain completely protected from the negative effects of radiation.
Radiation therapy is carried out in sessions (fractions), each lasting no more than 20 minutes. The treatment is outpatient (without hospitalization) and does not require special preparation of the patient in the form of anesthesia and pain relief.
How does IMRT radiation therapy differ from less precise radiation treatments for throat cancer?
IMRT technology makes it possible to deliver the required amount of radiation precisely to the boundaries of the tumor, regardless of the complexity of its shape, as well as to simulate the shape of the fields and the general area in such a way as to exclude irradiation of critical structures of the body (for example, in the treatment of laryngeal cancer, this is the spinal cord, salivary glands, muscles larynx and other vital organs.
Controlled step-by-step delivery of the required therapeutic dose of ionizing radiation (leading to damage to tumor tissues) to a specified volume. This principle is used to treat not only laryngeal cancer, but also all tumors, regardless of their size and location in the patient’s body.
The accuracy of treatment is achieved by preliminary modeling of the location of the tumor and healthy tissue around it, performed on the basis of CT and MRI images. After creating the model, the radiologist identifies the contours of healthy tissues with varying degrees of permissible radiation exposure, and areas of tumor damage. At the next stage, the radiation therapist enters into the system the values of the minimum and maximum radiation doses that must be delivered to each group of tissues during the treatment process.
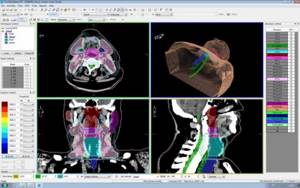
What does a radiation therapy plan for laryngeal cancer look like (photo)
Based on the given goals and limitations, the medical physicist creates in a special program a plan for delivering multiple radiation fields of complex shape. A high dose of radiation, lethal to tumor cells, but not leading to irreversible damage to healthy tissues, consists of zones of mutual intersection of fields. In this case, healthy tissues located along the path of each field will receive an even smaller dose.
The course of treatment for laryngeal cancer using a high-precision linear accelerator consists, on average, of 20-30 daily radiation therapy sessions of 15-20 minutes each. During the procedure, which is performed on an outpatient basis, without hospitalization, the patient lies in a comfortable position, his head is fixed with an elastic individual mask, which avoids significant movements and displacements of the radiation fields. Due to the non-invasive nature of the radiation treatment method, after the session the patient can return to his usual daily schedule.
Chemotherapy
In most cases, treatment for throat cancer involves the use of chemotherapy. When cancer cells are highly sensitive to chemotherapeutic drugs, chemotherapy at the beginning of combined treatment allows to reduce the volume of the malignant neoplasm before surgery. Chemotherapy can also be carried out in parallel with radiation therapy and after the surgical and radiation stages of treatment.
- Nutrition during chemotherapy
- Placing chemotherapy ports
Benefits of MRI
The advantages of the technique include harmlessness compared to ionizing radiation, non-invasiveness, high information content - it allows you to examine the smallest structures. The study helps not only to find a tumor, but also to determine its size, location, structure, degree of vascularization, contours, etc.
To make an appointment, use the form on the website or call us. MRI is a harmless technology, so there are no restrictions on the number of studies performed per year.
Risk factors
The risk of developing laryngeal cancer is high in smokers over the age of 55. You also need to know that drinking alcohol at the same time as smoking significantly increases the risk of developing the disease. The disease occurs four times more often in men than in women (the most common cancers among women are breast cancer and cervical cancer).
The risk of the disease is also increased in persons who have had or are suffering from head and neck cancer (in particular, thyroid cancer), as well as in those whose occupation is associated with the production of sulfuric acid, nickel, and asbestos.
Symptoms
Symptoms of laryngeal cancer have their own characteristics for each type of laryngeal cancer. The first signs of cancer depend on the part of the larynx that affects the tumor.
- Cancer of the vestibular larynx
At the initial stage, cancer develops almost asymptomatically, and the first manifestation of the disease is mild discomfort when swallowing; problems may not arise from the mucous membrane. Further growth of the tumor leads to a sensation of the presence of a foreign body, then to increasing pain when swallowing. Late stages of cancer (stage 3 and 4) of the vestibular larynx are characterized by the spread of pain when swallowing into the ears, which is why the patient limits the amount of food he eats and loses weight.
- Midlarynx cancer
Changes in voice and hoarseness are characteristic signs of cancer of the middle part of the larynx. Such symptoms may occur at the initial stage, with a small tumor. Hoarseness develops as the size of the tumor increases to the point of complete loss of voice. The late stage is also characterized by difficulty breathing.
- Subglottic cancer of the larynx
With this localization, the tumor compresses the vocal cord or grows into it (vocal cord cancer). This explains hoarseness that is not associated with colds. Less commonly, there is compression or blocking of the lumen of the larynx, which causes the patient to have difficulty breathing. Subsequently, tumors of this location can spread to the first rings of the patient’s trachea.
A significant proportion of patients are admitted with damage to two or three parts of the larynx. In such cases, symptoms of damage to various parts are observed simultaneously.
You should not look for photos of throat cancer on the Internet, and if you experience any alarming symptoms of the disease, you should immediately consult a doctor.
Doctor's second opinion
The larynx, nasopharynx and esophagus are not organs that can be correctly assessed by any doctor. Thus, a thorough and attentive analysis of CT or MRI images is extremely important because it allows you to answer questions that are important when choosing treatment methods. For example, is the tumor located in the subglottic space or supraglottic? What is its stage, is there any germination of the surrounding tissue? Is there damage to regional lymph nodes? In order not to make a mistake in diagnosis, you can resort to a Second Opinion and send the research results for consultation with a highly specialized diagnostician. Otherwise, analysis of CT or MRI images may be fraught with errors. Today you can send images for consultation using various medical services, such as the National Teleradiological Network.
Non-radiation methods for diagnosing the larynx
External examination and palpation of the larynx and neck area determines the volume, shape, consistency, degree of mobility of the larynx, the presence of pathologically changed and enlarged lymph nodes of the neck
Indirect laryngoscopy using a speculum determines the boundaries, location, shape and approximate size of the tumor.
Fibrolaryngoscopy, based on the use of special optics with flexible tubes, allows you to better assess the tumor and the condition of the larynx, as well as take material for a biopsy.
Fine-needle biopsy of the tumor and tissue examination of the biopsy is the most reliable method for confirming laryngeal cancer, as well as establishing its histological type.
Histological variants of laryngeal tumors
Based on their tissue structure, laryngeal tumors are classified as follows:
Laryngeal cancer
- Squamous (predominant variant)
- Adenocarcinoma (rare variant)
Sarcoma of the larynx
- Round cell sarcoma
- Carcinosarcoma
- Myosarcoma
- Chondrosarcoma
- Fibrosarcoma
- Lymphosarcoma
Secondary tumors
- Metastases of cancer and sarcoma of various localizations in the larynx. Mainly contact metastases in cancer of the esophagus, secondary tumor lesions of the mediastinal lymph nodes, lymphoma
- Downward spread of the pharyngeal tumor into the larynx is also possible
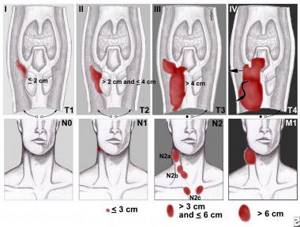
Staging of laryngeal cancer using the TNM system