What is folliculometry?
Pelvic ultrasound
women may be prescribed
folliculometry
- a dynamic study of the growth of the dominant follicle in the ovary. This procedure also allows you to determine the structure and thickness of the endometrium (the mucous membrane in the uterine cavity), which is necessary to ensure normal attachment of the fertilized egg. During folliculometry, the patient undergoes several dynamic ultrasounds to answer two main questions:
- Is the patient ovulating?
- Is the mucous layer of the uterus ready to attach the fertilized egg?
To conduct ultrasound folliculometry
, as practice shows, the patient must visit the doctor 3 to 5 times during one menstrual cycle (the doctor determines which specific days to do the examination). It is possible to prescribe more ultrasounds, depending on the dynamics of follicle growth.
When is folliculometry prescribed?
Folliculometry may be prescribed to women for the following purposes:
- identify/exclude pathology of ovarian function;
- assess the readiness of the endometrium to attach a fertilized egg;
- confirm/refute the presence of ovulation;
- assess the possibility of multiple pregnancy;
- determine all possible causes of menstruation or folliculogenesis (the process of follicle formation);
- assess the general hormonal levels in the patient’s body;
- identify/exclude pelvic diseases;
- assess the general condition of the woman’s reproductive system.
Folliculometry often precedes the IVF procedure - it is necessary to monitor the condition of the uterus and endometrium during the period of stimulation of ovulation. Folliculometry is also prescribed to monitor the results of therapy aimed at eliminating factors of infertility or pathology of the organs of the female reproductive system (cyst, fibroid, etc.).
What does folliculometry show?
Folliculometry shows the readiness of a woman’s reproductive system to conceive a child. An ultrasound will show whether ovulation has occurred. If yes, when did it happen? Folliculometry also shows the dynamics of the functional development of the endometrium, changes in its structure and thickness.
Signs of ovulation
- Registration of a “dominant” mature follicle immediately before ovulation.
- Reduction of the follicle in size, deformation of its walls, complete disappearance.
- After a few days, a corpus luteum, the size of which does not exceed 20 mm, forms in the ovary from which the egg was released.
- The presence of free (follicular) fluid in the posterior uterine space.
To confirm pregnancy, a week after ovulation, a woman’s blood is taken for progesterone. If progesterone is higher than normal, it means ovulation has occurred.
How is folliculometry done?
There are certain recommendations about what day of the menstrual cycle you should do ultrasound folliculometry. If the patient’s monthly cycle is 28 days, then the first examination is done on days 7-10 of the cycle. Further ultrasounds are scheduled at intervals of 1-2 days (here everything depends on the results of each previous ultrasound). If the patient’s monthly cycle lasts longer than 28 days, then the first ultrasound is scheduled on the 10-12th day of the cycle. If the cycle is shorter than 28 days, the first ultrasound examination can be performed on the 3-5th day. Further, intervals of 1-2 days are also observed.
Features of embryonic development after IVF
In the first 20 days from conception, the embryo undergoes major changes, ranging from gastrulation to organogenesis. During the embryonic period, which begins from the moment of fertilization until the 10th week of obstetrics, the embryo rapidly increases in size.
At 2 and 3 weeks of gestation, the embryo does not resemble a baby and only at the stage of organogenesis gradually acquires characteristic shape and structure. In the last week of the embryonic period, the gill arches and tail disappear in the fetus.
Embryos at 20 days after conception
- On the ninth day after implantation into the wall of the uterus, the process of cell division of the embryo continues, as a result of which it is transformed from a single-layer blastosphere into a gastrula with several embryonic petals;
- On days 20-21, the embryo enters the neurula stage, which is characterized by the formation of the neural plate;
- At the beginning of the 4th week of gestation, the process of placenta formation begins. The chorion and amnion arise from the ectoderm and trophoblast, in which amniotic fluid subsequently begins to accumulate.
The chorion is a villous formation that produces hCG. With the participation of the mesoderm, a fetal place is formed from it, in which the fetus continues further development. By the end of the third week of gestation, the fetus reaches only 4-5 mm in length and looks more like an oblong cylinder.
Decoding the results
Immediately after the ultrasound, the doctor begins to decipher its results. Normally, the follicle should look like a vesicular, echo-negative formation. As a rule, the first ultrasound shows the presence of several small follicles in the patient. Normal follicle growth is 2-3 millimeters per day. Before entering the egg, the size of the follicle should be 1.8-2.3 cm.
When the vesicular structure of the follicle disappears, a cystic formation and free fluid appear in the space behind the uterus, the fact of ovulation is diagnosed. In this case, we can conclude that the woman’s reproductive system is ready for conception.
When there is no ovulation, the doctor will have to figure out the possible reasons for this deviation:
- Fusion of the follicle (atresia) is a sudden cessation of growth of the dominant follicle after reaching a size of 1.8 cm with a further decrease in the size reached.
- Persistence is the normal development of the follicle, but at the same time the absence of the fact of its rupture and the release of the egg from it. In such a situation, hormonal imbalance is most often diagnosed, that is, the absence of the release of the hormone progesterone.
- Follicle cyst. This condition is a consequence of persistence. The growth of the follicle does not stop; fluid accumulates in it. A follicle cyst is diagnosed when its size exceeds 2.5 cm.
- Luteinization is the premature formation of the corpus luteum in the ovary.
An ultrasound may also show a complete absence of follicle formation. This condition is called anovulation, in which pregnancy is impossible.
What does a follicular cyst look like on an ultrasound?
A follicular cyst on ultrasound looks like a small tumor with a liquid component, which forms in the ovarian tissue, but does not have its own histological capsule.
An important question: “How to distinguish a follicle from a cyst on ultrasound?” It all depends on the individual characteristics of the patient’s body. It is necessary to evaluate the structure of the follicle and its size. If the follicle size is 27-28 mm or more, a cyst can be diagnosed, but dynamic observation - folliculometry - must be continued.
As practice shows, it can be quite difficult to distinguish a follicle from a cyst on an ultrasound. It is necessary to contact experienced diagnosticians who work with modern, multifunctional ultrasound equipment.
Female reproductive system: a little physiology
Ovaries (lat. ovarium) are paired female genital organs in which the development and maturation of the egg occurs.
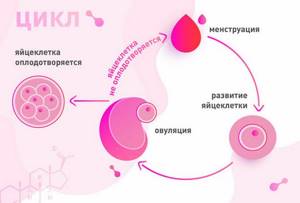
At the beginning of the menstrual cycle, follicle-stimulating hormone is produced. This hormone stimulates the ovaries to synthesize follicles that contain immature eggs, and also promotes the production of estrogen. The follicular apparatus is formed during the intrauterine development of the fetus.
As a rule, one of these follicles becomes “dominant” and when the required size (15-18 mm) is reached, the development of the remaining follicles stops and their atresia (reverse development) begins. Soon the “dominant” follicle bursts, releasing a mature egg, which leaves the ovary. This is ovulation.
On the day of ovulation, there is a decrease in basal temperature, an increase in progesterone levels, and an abundance of vaginal discharge. In rare cases, a woman may feel a short-term nagging pain in the lower abdomen. When there are hormonal imbalances in the body, the follicle does not rupture, or follicles are not synthesized at all. Ultrasound folliculometry is an informative diagnostic that helps monitor egg maturation.
Diagnosis for anovulation
Problems with ovulation are a phenomenon that must be treated if a woman expects to become a mother. But for this it is necessary to establish precisely whether such a condition really exists, and also what caused it.
The presence of pathology is indicated by the following symptoms of lack of ovulation:
- changes in the duration, intensity and nature of menstrual bleeding, as well as the interval between menstruation;
- dysfunctional uterine bleeding;
- rare or completely absent menstruation;
- male pattern body hair (hirsutism);
- hair loss, appearance of acne (acne);
- painful sensations in the mammary glands;
- pathological growth of the endometrium and some other gynecological pathologies.
The very presence of these signs (or some of them) is indirect evidence confirming anovulation. To make an accurate diagnosis and determine the cause of the pathology, a woman undergoes a series of diagnostic procedures;
- examination and consultation with a gynecologist, medical history;
- measurement of basal temperature - normally it increases by 0.2-0.4 degrees (above 37 degrees) in the 2nd (ovulatory) phase of the menstrual cycle, and during anovulation the temperature graph is even.
- blood tests for hormone levels (LH, FSH, 17-OP, prolactin, testosterone, cortisol, thyroid hormones);
- radiography of the skull, in particular the area where the pituitary gland is located (sella turcica);
- Ultrasound of the pelvic organs, mammary and thyroid glands.
Diagnosis in the absence of ovulation is complex, since often this pathology is caused by several reasons that are rooted in various organs and systems of the female body.
Types of folliculogenesis disorders
Unfortunately, folliculogenesis often goes wrong, which affects a woman’s health and ability to conceive a child. Ultrasound of folliculogenesis can provide the following information confirming a folliculogenesis disorder:
- regression (atresia) of the follicle. The dominant follicle was visualized, developed, and then abruptly stopped developing and began to shrink, as a result of which ovulation did not occur;
- Follicle persistence is a violation of folliculogenesis, which is characterized by the absence of rupture of the follicle and, accordingly, the release of the egg. With this pathology, the follicle can exist throughout the entire cycle, as well as after menstruation;
- follicular cyst. The dominant follicle grows to the required size, but does not rupture. Subsequently, follicular fluid accumulates in it and a cyst forms;
- luteinization of the follicle. This is a disorder of folliculogenesis, in which the corpus luteum is formed in the absence of rupture of the follicle. The reason may be a premature increase in hormones that affect ovulation, or a pathology of the ovarian structure;
- lack of follicular development is a case when there is no development of the dominant follicle, which is why ovulation is impossible.
If monitoring of folliculogenesis shows that ovulation does not occur for one of the above reasons, the doctor prescribes additional studies and tests. Then, based on the test results, treatment is prescribed, the purpose of which is to normalize hormonal levels and stimulate ovulation.
folliculogenesis, ovulation