The disease, which was called “pernicious anemia” (pernicious or B12 deficiency anemia) and which is characterized by a decrease in red blood cells and hemoglobin in the blood, was first described in the 19th century. It was considered contagious, incurable, and over its long history has claimed many hundreds of thousands of lives. It was only in the 20th century that scientists reported that anemia could be treated by introducing raw liver into the human diet, for which they received a Nobel Prize. But the substance itself, contained in the liver and saving people from anemia, could not be isolated for a long time.
In the mid-twentieth century, American and English scientists independently isolated red crystals of a substance that was given the name “vitamin B12,” but only in 1973 were they able to synthesize an artificial vitamin.
Mechanism of B12 Absorption
B12 is synthesized in nature by soil microorganisms, inhabitants of root crops and legumes, and is present in the muscles, liver, and kidneys of animals that feed on these plants. Humans get B12 from animal foods.
In order for vitamin B12 to be absorbed in the human body, and this happens at the very end of the small intestine, the vitamin from food must combine in the stomach with the so-called intrinsic Castle factor - a substance that is secreted by stomach cells that produce acid in the stomach and is a carrier of vitamin B12 to the site suction. Low acidity of gastric juice interferes with the absorption of B12. In addition, calcium is required for the absorption of B12 in the intestine.
The total content of B12 in humans, mainly in the liver, is 2-5 mg. Daily expenditure is 2-5 mcg (micrograms) per day. If the intake of B12 from animal foods is completely stopped, anemia will develop in 3-4 years, which is observed in vegetarians. But this is already a pronounced and irreversible process.
Detailed description of the study
Vitamin B12 (cyanocobalamin) is a biologically active substance necessary for humans, which contains the coenzyme cobalamin. The vitamin is not produced in the body; it comes only from food of animal origin. Foods with the highest levels of vitamin B12 include liver, eggs, meat, cheese and milk.
Getting into the lumen of the gastrointestinal tract along with food, vitamin B12 is absorbed in the small intestine (ileum). After absorption, cyanocobalamin enters the liver, where its reserves are stored. The daily requirement for vitamin B12 is 1-3 mcg, and its reserves in liver cells can reach 3000-4000 mcg. This explains the fact that diseases associated with B12 deficiency develop gradually.
The main functions of vitamin B12 in the body:
- Participation in the growth and maturation of erythrocytes (red blood cells);
- Maintaining normal metabolism of organic (fatty) acids in nervous tissue cells;
- Regulation of glucose metabolism;
- Participation in the formation of cell DNA (regulation of the process of their division);
- Maintaining the function of the immune, nervous and muscular systems.
In the first case, B12 deficiency leads to the formation of abnormal, reduced DNA size of red blood cells - the processes of division and maturation of red blood cells are disrupted. Such red blood cells are called megaloblasts - these cells are large in size and have a fragile membrane, which is why their lifespan is usually reduced by three times (30-40 days instead of 100-120). As a result, B12 deficiency or pernicious anemia develops.
In the second case, cyanocobalamin deficiency leads to the accumulation of a toxic metabolite (methylmalonic acid), which destroys the myelin sheath of nerve fibers.
The main cause of insufficient levels of vitamin B12 is not a malnutrition, but a deficiency of intrinsic factor due to atrophic gastritis, alcohol abuse and gastric removal/resection surgery. Normally, the factor is produced by the parietal cells of the stomach and promotes the absorption of B12 in the small intestine. It ensures normal absorption of cyanocobalamin from food - in its presence, about 70% of vitamin B12 is absorbed, in its absence - 2% of all molecules. Intestinal diseases that impair absorption also contribute to B12 deficiency.
The main symptoms of B12 deficiency anemia include:
- Inflammation of the tongue (glossitis), often affecting the edges or tip of the tongue. Further, glossitis subsides, the tongue takes on a shiny “varnished” appearance;
- Pale skin, mild jaundice (against the background of anemia and the release of hemoglobin into the blood);
- Decreased appetite (especially for meat products);
- Increased size of the liver and/or spleen (in 25% of cases);
- The stool is deep brown in color.
Also, with low B12 levels, patients with anemia may develop neurological symptoms:
- Feeling of tingling, numbness, coldness in the legs (rarely in the arms);
- Muscle weakness;
- Reduced pain and temperature sensitivity;
- Mental disorders and persistent paralysis are observed in severe cases.
B12 deficiency anemia usually develops in people over 65 years of age, as well as in people who abuse alcohol. The latter are often deficient in other B vitamins (B1, B6 and B9). A deficiency of cyanocobalamin in the body can be suspected if inflammation of the tongue develops, skin becomes pale and slightly jaundiced. The study of B12 in the blood allows you to establish the correct diagnosis in differential diagnosis with other (macrocytic) anemias with a similar course.
In the laboratory department of "Hemotest" you can take a test for vitamin B12 (total), as well as its active form - holotranscobalamin - with subsequent interpretation of the result.
B12 deficiency anemia. Symptoms
With a lack of vitamin B12, a person initially worries about weakness, fatigue, decreased performance, irritability, and headache.
Further, areas of inflammation appear on the tongue, which then covers the entire surface of the tongue, the tongue becomes “crimson” (“scalded”), ingestion of food and medications is accompanied by a burning sensation and pain in the oral cavity, heaviness in the epigastric region and loss of appetite appear. Prescribing heartburn medications to patients in this situation is not only not indicated, but is also dangerous due to its consequences - the development of pernicious anemia.
In the later period, memory deterioration, tinnitus, palpitations, shortness of breath during exercise, pain in the heart area, swelling in the legs are observed, which allows doctors to assume that the patient has coronary heart disease. With B12 deficiency, damage to the peripheral nerves, spinal cord and brain occurs - anxiety, depression, and psychosis occur.
The predominant age of patients is over 60 years, but vitamin B12 deficiency can occur in people of any age. It often occurs against the background of existing gastritis with reduced or absent hydrochloric acid and enzymes, and can accompany stomach cancer. B12 deficiency anemia develops acutely in the presence of concomitant factors - celiac disease, chronic alcoholism, taking certain medications, for example, aminosalicylic acid (aspirin), metformin, oral contraceptives and others, with prolonged heat treatment of foods. The unused vitamin is excreted in the bile, which makes it possible for it to be reabsorbed into the blood if it is deficient in food. After removal of the gallbladder, this process is disrupted and vitamin B12 is lost in the stool.
B12 deficiency anemia
The role of cyanocobalamin and folic acid in the development of megaloblastic anemia is associated with their participation in a wide range of metabolic processes and metabolic reactions in the body. Folic acid in the form of 5,10 - methylenetetrahydrofolate is involved in the methylation of deoxyuridine, necessary for the synthesis of thymidine, resulting in the formation of 5-methyltetrahydrofolate. Cyanocobalamin is a cofactor in the methyltransferase catalytic reaction that resynthesizes methionine and simultaneously regenerates 5-methyltetrahydrofolate into tetrahydrofolate and 5,10 methylenetetrahydrofolate.
With a deficiency of folate and (or) cyanocobalamin, the process of incorporation of uridine into the DNA of developing hematopoietic cells and the formation of thymidine are disrupted, which causes DNA fragmentation (blocking its synthesis and disrupting cell division). In this case, megaloblastosis occurs, accumulation of large forms of leukocytes and platelets occurs, their early intramedullary destruction and shortening of the life of circulating blood cells. As a result, hematopoiesis is ineffective, and anemia develops, combined with thrombocytopenia and leukopenia.
In addition, cyanocobalamin is a coenzyme in the conversion of methylmalonyl-CoA to succinyl-CoA. This reaction is necessary for the metabolism of myelin in the nervous system, and therefore, with cyanocobalamin deficiency, along with megaloblastic anemia, damage to the nervous system is noted, while with folate deficiency, only the development of megaloblastic anemia is observed. Cyanocobalamin is found in food products of animal origin - liver, kidneys, eggs, milk. Its reserves in the body of an adult (mainly in the liver) are large - about 5 mg, and if we take into account that the daily loss of the vitamin is 5 mcg, then complete depletion of reserves in the absence of intake (malabsorption, with a vegetarian diet) occurs only after 1000 days . Cyanocobalamin in the stomach binds (against the background of an acidic environment) with an intrinsic factor - a glycoprotein produced by the parietal cells of the stomach, or other binding proteins - R-factors present in saliva and gastric juice. These complexes protect cyanocobalamin from destruction during transport through the gastrointestinal tract. In the small intestine, at an alkaline pH, under the influence of pancreatic juice proteinases, cyanocobalamin is cleaved from R-proteins and combines with intrinsic factor. In the ileum, the complex of internal factor with cyanocobalamin binds to specific receptors on the surface of epithelial cells, the release of cyanocobalamin from intestinal epithelial cells and transport to tissues occurs with the help of special blood plasma proteins - transcobalamins 1,2,3, and the transport of cyanocobalamin to hematopoietic cells is carried out predominantly transcobalamin 2.
Folic acid is found in green plant leaves, fruits, liver, and kidneys. Folate stores are 5-10 mg, the minimum requirement is 50 mcg per day. Megaloblastic anemia can develop after 4 months of complete lack of dietary folate intake.
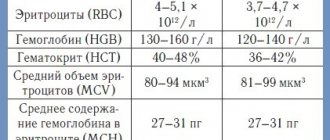
B12 deficiency anemia. Diagnostics
Diagnosis of vitamin B12 deficiency is not always easy, since at the onset of the disease the clinical manifestations are not very specific.
Vitamin B12 deficiency is reliably determined by low levels of B12 in the blood plasma. However, a normal level of B12 is often determined in the plasma due to the fact that for any anemia the patient is given vitamin preparations containing vitamin B12 and folic acid. People's commitment to prophylactic intake of complex vitamin preparations is also high. In this case, B12 deficiency anemia is not diagnosed, and its characteristic signs disappear. Vitamin B12 treatment should not be started before a diagnosis has been made.
References
- Demikhov, V.G., Skobin, V.B., Zhurina, O.N. and others. Federal clinical guidelines for the diagnosis and treatment of anemia caused by B12 deficiency, 2014. - 8 p.
- Clinical oncohematology: a practical guide / ed. M.A. Volkova M.A., 2001. -576 p.
- Arthur, C., John, E. Textbook of Medical Physiology. 13th Edition, 2015. - p. 980-987.
- Kumar, V., Abbas, A., Aster, J. Robbins and Cotran Pathologic Basis of Disease, 2014. - Vol. 1(9). — 1408 p.
- O'Leary, F., Samman, S. Vitamin B12 in health and disease. Nutrients, 2010. - Vol. 2(3). — P. 299-316.
B12 deficiency anemia. Treatment
Treatment at first glance is simple - B12. But the whole question is what is the cause of your B12 deficiency, how to get B12 to the right place, how to make it work and how long should you take it. B12 tablets cannot cure pernicious anemia!
Injections of B12 are given according to a specific regimen in combination with other vitamins and minerals selected by the doctor.

It is important to know the sources of vitamin B12 in food products per 100 g:
- beef liver -60 mcg (microgram),
- pork liver – 30 mcg,
- herring – 18.7 mcg,
- chicken liver - 16.58 mcg,
- mackerel - 12 mcg,
- sardines - 11 mcg,
- sea bass - 2.4 mcg,
- shrimp, mussels – 8-20 mcg,
- cod, carp, cheese - 1.6-1.4 mcg,
- chicken, eggs, milk and dairy products - less than 0.6 mcg.
- Plant foods do not contain vitamin B12.
What else is prescribed with this study?
B vitamins (B1,B2,B3,B5,B6,B9,B12)
4.23.1. Venous blood 7 days
RUB 10,590 Add to cart
Homocysteine
1.53. Venous blood 1 day
RUB 1,150 Add to cart
Complete blood count without leukocyte formula (venous blood)
3.1.1. Venous blood 1 day
190 RUR Add to cart
Folates
4.3. Venous blood 1 day
750 RUR Add to cart
Interesting facts about vitamin B12
- The intestinal microflora synthesizes vitamin B12. As a result, the consumption of fermented milk products and preparations of live bacteria contribute to the normal content of intestinal microflora, although the amount of vitamin they produce does not cover the body's needs.
- If a person has a harmless passion for sweets, then the own microflora of the intestinal tract changes, putrefactive bacteria, fungi, and parasites appear, which begin to lay claim to vitamin B12, which comes with food.