Thanks to multislice computed tomography of the chest, or MSCT, which is considered the most informative method of examining the lungs, doctors can diagnose infectious, inflammatory and oncological diseases in the early stages.
“Frosted glass” is characteristic of pneumonia, tuberculosis, lung cancer and other dangerous conditions. Which ones exactly and by what characteristics are they distinguished? Let's take a closer look in this article.
Pulmonary edema is
Pulmonary edema is a pathological condition in which a sharp disruption of gas exchange in the lungs occurs and hypoxia develops - a lack of oxygen in organs and tissues.
The lungs swell due to a sharp increase in pressure in the blood vessels, insufficient protein, or the inability to retain water in the liquid part of the blood that does not contain cells - plasma. Pulmonary edema is manifested by shortness of breath at rest, a feeling of tightness in the chest, suffocation, cyanosis, cough with foamy bloody sputum, bubbling breathing. Diagnosis of pulmonary edema involves auscultation, radiography, ECG, echocardiography. Treatment of pulmonary edema requires intensive therapy, including oxygen therapy, administration of narcotic analgesics, sedatives, diuretics, antihypertensive drugs, cardiac glycosides, nitrates, and protein drugs.
3.Diagnostics of interstitial lung diseases
Typically, people with interstitial lung diseases come to a pulmonologist for consultation with complaints of shortness of breath or cough. To make a diagnosis, the doctor usually uses special methods of examining the lungs.
:
- Chest X-ray. This test is usually done first to evaluate the overall health of the lungs. Interstitial lesions may appear on imaging as fine lines in the lungs.
- Computed tomography (CT). Tomography allows you to create a detailed image of the lungs and adjacent structures. Interstitial lung diseases are typically seen on CT scans.
- High resolution CT. Special tomograph settings for suspected interstitial disease increase diagnostic efficiency.
- Assessment of external respiratory function using special lung tests, including body plethysmography, spirometry and some others.
- Lung biopsy and examination of the resulting samples under a microscope. This is often the only way to determine what type of lung tissue damage a patient has. Biopsy tissue samples can be taken using bronchoscopy, video-assisted thoracoscopic surgery, or open lung biopsy (thoractomy).
About our clinic Chistye Prudy metro station Medintercom page!
Classification of the disease
Pulmonary edema, depending on the cause of its occurrence, is divided into two types:
- Hydrostatic, which is characterized by the formation of the disease based on an increase in intravascular hydrostatic pressure. With hydrostatic edema, fluid is removed from the vessel into the alveolus. Hydrostatic pulmonary edema often occurs due to cardiovascular insufficiency.
- Membranous, manifests itself due to the influence of toxins, resulting in destruction of the walls of capillaries and alveoli. This gives impetus to the entry of fluid into the intravascular space.
Pulmonary edema also has two forms of complications, which have corresponding symptoms and signs of the disease. These forms of complications are called:
- Alveolar.
- Interstitial.
Of these two forms, it is worth highlighting the first (alveolar), since it is the most dangerous and leads to dire consequences, in particular, to human death. Interstitial, in turn, is a more gentle form that is subject to treatment and successful recovery. If you do not take appropriate therapeutic measures, then this form worsens and becomes alveolar.
Pulmonary edema has another type of classification: according to the severity of manifestations. There are four degrees, which are characterized by the following signs of manifestations:
- The first degree is called pre-edema and is characterized by the appearance of mild signs of shortness of breath and disturbances in the frequency and rhythm of breathing.
- The second degree is medium, which is characterized by the appearance of wheezing. Shortness of breath increases.
- Third degree - the disease becomes severe and is characterized by increased shortness of breath and wheezing, which can be heard even at a distance.
- Fourth degree - immediate symptoms of the disease occur: weakness, sweating, wheezing, etc. More details about the symptoms in the disease symptoms section.
Symptoms of pulmonary edema
The main symptoms of pulmonary edema include:
- frequent coughing;
- increasing hoarseness;
- cyanosis (the face and mucous membranes become bluish);
- increasing suffocation;
- tightness in the chest, pressing pain;
- increased breathing;
- dizziness, weakness;
- bubbling wheezing is heard;
- with increasing cough - foamy pink sputum;
- as the condition worsens, sputum is released from the nose;
- the person is scared, consciousness may be confused;
- sweating, cold and sticky sweat;
- fear of death;
- increased heart rate up to 200 beats per minute. Can easily develop into life-threatening bradycardia;
- drop or surge in blood pressure.
The leading symptom of pulmonary edema is suffocation. If you have difficulty breathing, you should immediately contact a specialist.
Pulmonary edema itself is a disease that does not occur on its own. Many pathologies can lead to edema, sometimes completely unrelated to diseases of the bronchopulmonary and other systems
2. Causes and symptoms of diseases
Causes of interstitial lung diseases.
The causes of damage to lung tissue can be different. So, interstitial pneumonia
may be caused by bacteria, viruses or fungus.
Other interstitial diseases may be associated with regular inhalation of irritating substances
- asbestos, quartz dust, talc, coal and metal dust, grain dust.
In rare cases, lung diseases in this group may develop due to exposure to certain drugs
.
The peculiarity of interstitial lung diseases is that the above factors, in fact, cause only some of the diseases. In most cases, the exact cause of lung disease remains unknown.
.
Symptoms of interstitial lung diseases.
The most common symptom of all forms of the disease is shortness of breath, which may worsen over time. In most diseases, shortness of breath develops quite slowly, over about a month. In the case of interstitial pneumonia or acute interstitial pneumonia, symptoms can develop very quickly, in just a few days or even hours.
Other symptoms of the disease may be
- The cough is usually dry and unproductive;
- Weight loss;
- Labored breathing.
Visit our Pulmonology page
Pulmonary edema in newborns
The causes of pulmonary edema in newborns are:
- Entry of amniotic fluid into the bronchi and alveoli.
- Death of cellular tissue of a certain area of the placenta or placental infarction. With this pathology, the blood supply to the fetus is disrupted and the likelihood of hypoxia is high.
- Heart defects. With narrowing of the arterial valve and mitral valve insufficiency, the pressure in the pulmonary circulation increases. These ailments provoke blood to enter the lungs and then into the alveoli.
- Brain injury during childbirth or prenatal, as a result of which the blood supply to the entire body is disrupted. As a result, oxygen starvation and, as a result, pulmonary edema.
When is a doctor needed?
Medical assistance is needed in any case, when the first signs of edema are detected, regardless of what caused it. In the vast majority of cases, urgent hospitalization is necessary.
If a patient is diagnosed with diseases of the cardiovascular system and experiences chronic and long-term pulmonary edema due to heart failure, it is necessary to constantly monitor the attending physician, follow all his recommendations and regularly undergo diagnostic and laboratory tests.
Regarding chronic pulmonary edema, constant monitoring by specialists is necessary:
- in internal medicine (therapist);
- for cardiovascular diseases (cardiologist);
- in pulmonary diseases (pulmonologist).
“Ground glass” for adenocarcinoma (cancer) of the lung
Based on the “ground glass” effect on a CT scan of the lungs, malignant neoplasms—lung cancer—are determined. Adenocarcinoma is the most common type of tumor; a significant “trigger” for its formation is smoking, heredity, and age (over 40 years).
Adenocarcinoma tumor is formed from glandular epithelial cells. On the tomogram it is represented by a single, usually small (from 2 mm) area of compaction of the “frosted glass” type. In some cases, the patient has several “frosted glasses” of a diffuse or diffuse mosaic type. Adenocarcinoma is presented in various morphological subtypes and requires dynamic monitoring.
Do not try to interpret the images yourself. Only a specialized doctor who has been trained and has the appropriate certificate can identify “frosted glasses” and give them a differentiated assessment.
Mechanism of edema development
Normally, lung tissue consists of many tiny air-filled bubbles called alveoli. If, in addition to air, liquid begins to accumulate in the alveoli - as a result of sweating from the circulatory and lymphatic systems - pulmonary edema occurs.
The mechanism of occurrence of this pathological condition is as follows:
- As a result of stagnation in the pulmonary circulation, the outflow of blood and lymph is disrupted and intravascular pressure in the pulmonary capillaries and lymphatic vessels increases.
- Blood and lymph accumulate in the vessels and begin to penetrate through their walls into the pulmonary structures of the alveoli - the so-called fluid effusion occurs.
- The liquid or transudate that has penetrated into the alveoli seems to displace air from them and significantly reduce their respiratory surface. The situation gets worse as the amount of transudate in the lungs increases - the effect of “internal drowning” is observed when the lungs fill with water and cannot fully function.
- Transudate is very rich in protein and therefore easily foams when in contact with air in the alveoli. The resulting foam makes breathing even more difficult.
- As a result, breathing becomes almost impossible, oxygen does not enter the blood, hypoxia and death occur.
Diagnostics
Diagnostic measures are determined depending on the patient’s condition.
Visual inspection. If the patient is conscious and can answer questions adequately, the doctor should begin collecting anamnesis. A detailed questioning is necessary in order to be able to establish the cause of the development of edema.
In case of loss of consciousness, the doctor pays attention to the color of the skin, the condition of the pulsating veins of the neck, breathing, heartbeat, and the presence of sweat. Percussion (tapping) of the chest and auscultation (listening with a phonendoscope) are performed. The doctor measures blood pressure.
Laboratory methods. A general blood test and biochemical blood test are performed.
Instrumental methods. If necessary, pulse oximetry (determining the degree of oxygen saturation of the blood), determination of central venous pressure values using a Waldman phlebotonometer, electrocardiography (ECG), echocardiography (ultrasound of the heart), and chest radiography are prescribed.
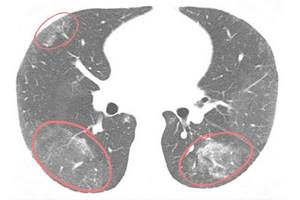
“Frosted glass” on CT scan for tuberculosis

Foci of infiltration of the “frosted glass” type are also found in tuberculosis. It is caused by the bacterium Mycobacterium tuberculosis. It is believed that all adults over 30 years of age are carriers of mycobacteria in a “dormant” form. When the immune system is suppressed, tuberculosis bacteria can become active and the person will become ill.
In tuberculosis, CT scans of the lungs usually show multiple small (miliary) lesions disseminated throughout the lungs. Their concentration in a certain proportion is possible. There is often an infiltrate in the form of a “path” leading to the root of the lung. There is an increase in lymph nodes. It is possible to definitively distinguish tuberculosis from pneumonia based on the results of PCR diagnostics - a blood test for the causative agent of infectious pneumonia.

Treatment of pulmonary edema
Treatment of pulmonary edema is carried out in the ICU under constant monitoring of oxygenation and hemodynamics. Emergency measures in the event of pulmonary edema include:
- giving the patient a sitting or half-sitting position (with the head of the bed raised), applying tourniquets or cuffs to the limbs, hot foot baths, bloodletting, which helps reduce venous return to the heart.
- It is more expedient to supply humidified oxygen during pulmonary edema through antifoam agents - antifomsilan, ethyl alcohol.
- if necessary, transfer to mechanical ventilation. If there are indications (for example, to remove a foreign body or aspiration of contents from the respiratory tract), a tracheostomy is performed.
- administration of narcotic analgesics (morphine) to suppress the activity of the respiratory center.
- administration of diuretics (furosemide, etc.) to reduce blood volume and dehydration of the lungs.
- administration of sodium nitroprusside or nitroglycerin to reduce afterload.
- the use of ganglion blockers (azamethonium bromide, trimethaphan) can quickly reduce pressure in the pulmonary circulation.
According to indications, patients with pulmonary edema are prescribed cardiac glycosides, antihypertensive, antiarrhythmic, thrombolytic, hormonal, antibacterial, antihistamine drugs, infusions of protein and colloid solutions. After stopping the attack of pulmonary edema, treatment of the underlying disease is carried out.
For pulmonary edema, the following medications are used, which are taken by the patient via the fastest route - intravenously.
- To eliminate foaming, oxygen inhalation is used, which must be combined with alcohol. To lower blood pressure, drugs are used: Dopamine or Dobutamine, which increase the heart rate.
- Reduction of pain symptoms is achieved with the help of Morphine.
- Nitroglycerin is administered intravenously in a ratio with saline solution.
- Diuretics are prescribed: Furosemide.
- If the disease is caused by a critically low heartbeat, then the drug Atropine is used.
- Glucocorticosteroids. Prednisolone is used for bronchospasms.
- If a blood test shows a low protein content, then an infusion of fresh frozen plasma is used.
- If signs of the predominance of infectious microorganisms are detected, then a group of antibiotic drugs is prescribed: Ciprofloxacin or Imipenem. The drug Dobutamine
If timely measures are taken, treatment is successful and the patient is discharged after 2–3 weeks, depending on the form of the disease. The above-mentioned drug treatment is general, so not all drugs will necessarily be prescribed. For each specific case, appropriate personal treatment is prescribed.
Consequences of pulmonary edema
When the swelling is stopped, it is too early to end the treatment. After an extremely severe condition of pulmonary edema, serious complications often arise:
- addition of a secondary infection. Pneumonia most often develops. Against the background of reduced immunity, even bronchitis can lead to adverse complications. Pneumonia associated with pulmonary edema is difficult to treat;
- hypoxia, characteristic of pulmonary edema, affects vital organs. The most serious consequences can affect the brain and cardiovascular system - the effects of swelling may be irreversible. Cerebral circulation disorders, cardiosclerosis, heart failure without powerful pharmacological support lead to death;
- ischemic damage to many organs and systems of the body;
- pneumofibrosis, segmental atelectasis.
How to help a patient with pulmonary edema?
The algorithm of actions for providing first emergency aid for pulmonary edema consists of performing the following emergency measures:
- Call an ambulance. You cannot ignore complaints and wait for the condition to worsen - pulmonary edema can lead to death almost instantly.
- Reassure the patient: use valerian or motherwort.
- Unbutton all clothing that restricts breathing.
- Sit on a chair, lower your legs down. Such a patient should not be placed in a horizontal position.
- Before the doctor arrives, you can apply tourniquets to the limbs that are compressing the veins. It is important not to allow the pulse to disappear on the clamped limb. The tourniquets are applied for 15-20 minutes and then removed. After some time they can be applied again. Thus, the heart is unloaded - it requires less effort to pump blood to the periphery of the body.
- You can give the patient 1 tablet of nitroglycerin sublingually.
- If possible, use an oxygen mask.
- If a large amount of foam is released during a cough, you should use antifoaming agents. At home, this can be ordinary alcohol: a towel soaked in vodka or medical alcohol is periodically applied to the patient’s nose and mouth. It is better not to use expectorants if the cough has already become wet with copious sputum.
- To prevent swelling from spreading, you should warm the patient’s back: apply mustard plasters.
Which method of diagnosing pulmonary edema to choose: MRI or CT
Selection Methods:
- X-ray,
- CT scan (preferred to detect signs of cardiac pulmonary edema).
What will chest x-rays show for pulmonary edema?
- Thickening of interlobular septa (Kerley lines)
- Fuzzy vascular pattern
- Formation of peribronchial couplings
- Thickening of the pleura
- Decreased inspiratory depth (reduced lung compliance)
- Hydrostatic pulmonary edema due to gravitational forces affects the lower parts of the lungs more and is usually central
- With increased permeability of the vascular wall, the distribution of edematous fluid in the lungs is also influenced by gravity, but the edema is peripheral
- With cardiogenic pulmonary edema, cardiomegaly, cranialization of the pulmonary blood flow, and accumulation of fluid in the pleural cavity are also noted.
- With pulmonary edema caused by overhydration, the ratio of pulmonary and systemic blood flow is 1:1, the shadow of the mediastinal vascular bundle is expanded, and the soft tissues (chest wall) are edematous.
Is CT scan of the lungs informative for edema?
- Changes are the same as on chest x-ray
- The method is more specific;
- CT also shows darkening of the posterobasal parts of the lungs in the form of a reticular pattern.
Distinctive signs of pulmonary edema
- Thickening of interlobular septa
- Fuzzy vascular pattern
- Formation of peribronchial couplings.