Osteochondrosis of the spine is considered one of the severe degenerative-dystrophic processes, which consists in the occurrence of degenerative changes in the intervertebral discs and the gradual involvement of adjacent vertebrae, intervertebral joints and ligaments in the process.
- Etiology and pathogenesis of osteochondrosis of the spine (ridge)
- Clinical symptoms
- Diagnosis of spinal osteochondrosis
- Treatment of spinal osteochondrosis
Spine development
Normally, the development of the spine continues until the age of 20-22. Ossification of different parts of the spine is carried out in the following order: upper cervical, mid-thoracic, cervical, lower thoracic, lumbar, sacral. The apophyses of the vertebrae become ossified from 8 to 15-16 years of age. Ossification of the CII vertebra occurs at the age of 4-6 years. Physiological curves of the spine are outlined between the ages of 2 and 4 years, and at 6 years they become distinct. The amount of cervical lordosis decreases up to 9 years. With age, there is a change in the orientation of the facets of the intervertebral joints. In early childhood, the facets have a relatively horizontal arrangement. The increase in the angle of inclination of the facets continues up to 10 years, until they assume a vertical position, after which they are able to limit the movement of the vertebrae [1].
Anatomical and functional features of the upper cervical spine
The cervical spine has characteristic structural and functional features.
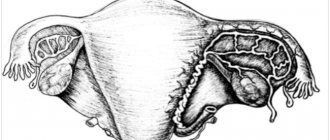
The first cervical vertebra, the atlas (CI), and the second cervical vertebra, the axis, or epistropheus (CII), connect the spine to the skull and form the atlantoaxial-occipital complex. The CI vertebra does not have a body, but there are anterior and posterior arches that limit the lumen of the spinal canal. The upper surface of the CI vertebra has slightly concave articular processes that are connected to the condyles of the occipital bone. Vertebra CII has a body that passes into the odontoid process. It protrudes upward, articulates with the inner surface of the anterior arch of the atlas and reaches the level of the foramen magnum. The CI vertebra is connected to the condyles of the occipital bone. There are three joints between vertebrae CI and CII: two paired joints between CI and CII and one between the odontoid process of CII and the arch of the CII vertebra (Fig. 1).
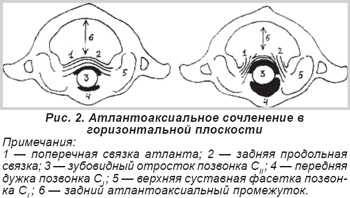
Functionally, these joints are combined into a combined joint, in which rotational movements of the head together with the CI vertebra are possible. Approximately half of all neck movements occur at the atlantooccipital and atlantoaxial joints. The articulation of the odontoid process with the atlas and the atlas with the occipital condyles is truly synovial. The joint capsules of these joints have a low degree of tension. The occipital bone is connected to the atlas by the occipitovertebral membrane, which is covered in front by the anterior longitudinal ligament. Between the posterior arch of the atlas and the edge of the foramen magnum is the posterior occipitovertebral membrane. Vertebral vessels and spinal nerves pass through it. The posterior longitudinal ligament is located on the posterior surface of the vertebral bodies. Below the posterior longitudinal ligament is the cruciate ligament, which consists of a transverse ligament and two crura. The ligament is stretched between the inner surfaces of the lateral masses of the CI vertebra on both sides. It wraps around the odontoid process, limiting its posterior displacement and thereby preventing compression of the spinal cord. Between the posterior surface of the odontoid process and the anterior surface of the ligament there is a mucous bursa. On the sides of the apex of the tooth lies a fatty lump, which protects the odontoid process from friction against the arch of the atlas. Under the cruciate ligament are the ligament of the apex of the odontoid process, which runs from it to the edge of the occipital foramen, and the pterygoid ligament, stretched between the lateral surface of the odontoid process and the articular processes of the occipital bone (Fig. 2).
In the spine, axial and rotational loads are placed on the vertebral bodies and intervertebral discs. Combined into a single structure, they ensure a vertical position of the body, withstand axial loads, absorb and distribute shock loads. Intervertebral discs connect the vertebrae to each other and provide the stabilizing function of the spine. Fixation of the intervertebral disc to the vertebral body is carried out by the fibers of the fibrous ring. The nucleus pulposus distributes the load applied to the spine. Intervertebral joints, reinforced by articular capsules, do not bear axial load. They determine the direction of movement of the vertebrae. Spinal ligaments fix the vertebrae and intervertebral discs together and influence the range of motion of the spine. The anterior longitudinal ligament prevents extension of the spine, the posterior longitudinal ligament, supraspinous, interspinous ligaments, as well as the nucleus pulposus limit flexion of the spine, intertransverse ligaments limit lateral bending [2]. Of all the ligaments of the spine, the anterior longitudinal ligament is the strongest. With age, the strength of ligaments decreases. The extensibility of the ligaments is most pronounced in places of maximum physiological kyphosis and lordosis, where vertical loads on the spine are absorbed. The greatest extensibility is found in the posterior longitudinal ligament in the cervical spine, which results in greater mobility. The ability of the vertebrae to move is related to their location and the direction of the shear force. The displacement at the level of the apex of lordosis and kyphosis occurs in the direction of the convexity of the curvature [1]. The mobility of the entire spine is the sum of movements of individual segments, which on average fluctuates within 4° [2]. The spine moves around three axes: 1) flexion and extension around the transverse axis, 2) lateral bending around the sagittal axis, 3) rotational movements around the longitudinal axis. Circular movements along all three axes are possible, as well as movements along the vertical axis.
Which is better - MRI, CT or X-ray for spinal osteochondrosis?
In addition to magnetic resonance imaging, osteochondrosis can also be diagnosed using a computed tomography scan of the spine or x-ray. All these types of studies will show whether a person has osteochondrosis. If you give preference to one of these forms of diagnosis, then, without a doubt, it will be an MRI of the spine. This scanning method, unlike radiation diagnostics, does not cause harmful radiation to humans. During the examination there is no x-ray radiation, no painful sensations. The diagnostic value of MRI images will also be higher than CT and X-ray tomograms. MRI for osteochondrosis will show not only the bone tissue of the vertebrae, but also connective tissue and articular cartilage.
Spinal instability
Instability is pathological mobility in the spinal segment. This can be either an increase in the amplitude of normal movements, or the emergence of new degrees of freedom of movement that are uncharacteristic for the norm. An indicator of spinal instability is the displacement of the vertebrae. Vertebral displacement is a radiographic finding, while spinal instability is a clinical concept. Displacement of the vertebrae can occur without pain, but instability is characterized by pain. Instability has characteristic signs:
1. Violation of the load-bearing capacity of the spine occurs when exposed to external loads, both physiological and excessive. The spine loses its ability to maintain certain relationships between the vertebrae.
2. Instability indicates the failure of the supporting complexes, which protect the spine from deformation, and the spinal cord and its structures protect from irritation.
3. The disorder manifests itself in the form of deformation, pathological movement of the vertebrae or destruction of the elements of the spine. Instability causes pain, neurological disorders, muscle tension and limitation of movement [3-5].
There are factors that predispose to excessive mobility of spinal segments. Normally, for the cervical spine, excess mobility is determined by two factors: age and vertebral location. The range of mobility of the spine in children exceeds the range of mobility in adults. The amplitude of displacement of the CI and CII vertebrae during flexion is 4 mm, and during extension – 2 mm [4]. Increased mobility of the CII-CIII segment is observed up to the age of 8 years [1]. In children, excessive mobility is observed in the upper cervical spine in 65% of cases [6], which is associated with the absence of an intervertebral disc at the CI-CII level. In children, the CII-CIII segment is the most mobile. Disorders at this level are diagnosed in 52% of cases of spinal instability [6].
The main symptom of instability is pain or discomfort in the neck. In the cervical spine in patients with instability in the atlanto-occipital joint, irritating pain can be periodic and intensify after physical activity. Pain is the cause of chronic reflex tension of the neck muscles. In children, instability is the cause of the development of acute torticollis. At the onset of the disease, there is increased tone of the paravertebral muscles, which leads to their overwork. Microcirculation disorders occur in the muscles, the development of malnutrition and decreased tone. There is a feeling of uncertainty when moving in the neck. The ability to withstand normal load is impaired. There is a need for means of additional immobilization of the neck, including supporting the head with the hands. In the clinic, cervical spine instability in adults is measured using a scoring system for assessing clinical signs (Table 1) [2].
Classification according to the degree of change in intervertebral discs
According to the degree of damage to the intervertebral discs, there are four stages of the disease, which are based on radiographic studies:
- Zero. With grade zero, there are no visible lesions in the spinal column.
- First. Internal disc ruptures without external changes.
- Second. The disc changes noticeably without external damage.
- Third. The intervertebral disc is severely affected. In this case, the cracks spread to the inner surface, and the disc itself is squeezed out of the vertebrae.
Radiological manifestations of instability
Normally, on a lateral projection radiograph, the posterior contours of the vertebral bodies form a regular arc. A manifestation of instability is displacement of the vertebrae. With instability, the continuity and smoothness of the line of the posterior contour of the vertebral bodies is disrupted, and the line itself acquires a bayonet-like deformity. The articular surfaces of the intervertebral joints lose their parallelism. An angle is formed between them, open anteriorly. These changes can be detected on standard radiographs, as well as on functional radiographs, which are taken in the position of maximum flexion and extension of the spine. Compared to a standard x-ray, in functional photographs the degree of vertebral displacement appears to be increased. Normally, with the maximum possible movements of the spine, a change in the height of the intervertebral discs is observed. With maximum flexion, the height of the anterior part of the disc decreases, and with extension, the height of the rear part of the disc decreases. A sign of instability is the convergence of adjacent areas of the vertebral bodies, which exceeds the boundaries of the physiological norm. Most often, spinal instability develops in areas of increased vertebral mobility. In the cervical region, these are the atlantoaxial and lower cervical levels. Subluxation is determined based on radiometric data from lateral radiographs. The x-ray is taken so that the lower part of the occipital bone and the hard palate are visible along with the cervical vertebrae. The relationships of the upper cervical vertebrae and the dimensions of the spinal canal are determined using a series of X-ray calculations (Fig. 3).
1. Determination of the posterior atlantoaxial space or longitudinal size of the spinal canal. This is the distance between the posterior surface of the odontoid process of the CII vertebra to the anterior surface of the arch of the CI vertebra. Normally it is 17±0.5 mm. A decrease in the size of the canal to less than 10 mm indicates anterior subluxation.
2. Determination of the anterior atlantoaxial space. This is the distance between the inner surface of the anterior arch of the CI vertebra and the anterior surface of the odontoid process of the CII vertebra (Cruvellier's joint). Normally, in an adult, when bending the head forward, this gap does not exceed 3 mm, and in a child, 5 mm. If this distance increases, anterior subluxation may be suspected.
3. McGregor's method. A line is drawn from the posterior edge of the hard palate to the anterior edge of the foramen magnum. The perpendicular to the center of the odontoid process is restored and the distance from this line to the apex of the odontoid process is measured. Normally it is 4-5 mm. An increase in this distance indicates vertical subluxation.
4. Ranawat method. A line is drawn through the center of the front and rear arms. The perpendicular to the center of the root of the CII vertebral arch is restored, which on the radiograph looks like a sclerotic ring. The distance from this line to the center of the bow is measured. Normally it is 15 mm. If this distance decreases, vertical subluxation is suspected.
5. Redlund-Ionell method. Distance between McGregor's line and the center of the lower edge of the CII vertebral body. For men this distance is 34 mm, and for women it is 29 mm. A decrease in this size indicates vertical subluxation.
Subluxation in the upper cervical region is of four types: 1) anterior, 2) posterior, 3) lateral, 4) vertical. Anterior subluxation is more common than all others. In an adult, a displacement of the CI vertebra by 3 mm is considered pathological. A displacement of 10-12 mm indicates destruction of the entire ligamentous complex. Lateral subluxation is determined if the displacement exceeds 2 mm. Subluxation is accompanied by lateral rotation of the head.
Normally, increased mobility in the lower cervical region is more common in segments CIII-CIV, CIV-CV and CV-CVI [6, 7]. Normally, the size of the spinal canal at level CIII ranges from 14 to 18 mm, and the displacement of the vertebrae in the anteroposterior direction is no more than 2 mm. This amount of displacement is relatively stable due to the preservation of the fixing function of the anterior longitudinal ligament.
Subaxial subluxations occur in the lower cervical spine. The earliest sign of instability is an increase in the angle between two adjacent vertebrae on functional radiographs. The most reliable sign of instability is a combination of vertebral displacement in the sagittal plane of more than 2 mm and the formation of an angle between the endplates of adjacent vertebral bodies of more than 10° (Fig. 4) [2].
Spinal instability may be accompanied by the development of kyphotic curvature of the spine. With degenerative instability, local kyphosis is observed in 40% of cases. It is a variable symptom of instability that can either worsen or disappear over time [5]. Increased mobility, characteristic of instability, occurs with almost the same frequency as lack of movement until its complete disappearance. Variants of spinal mobility impairment occur in different combinations:
1) increasing mobility at the level of instability;
2) decreased mobility at the level of instability in combination with increased mobility at the higher level;
3) decreased mobility in all segments of the spine [5].
Spinal instability is accompanied by the development of compensation. The severity of compensatory manifestations is associated with the degree of damage to the supporting structures of the spine, the intensity of the process of fibrotization of the disc, the age of the patient and the duration of the disease, the treatment performed, as well as the strength and tension of the muscles. When instability develops, the muscles perform the main compensatory work. There are two options for compensating for muscle instability:
1. Instability is compensated by muscle work. Muscle tension can keep the vertebrae from pathological movements, relieve the patient of discomfort and reduce the intensity of pain. The degree of compensation is proportional to muscle volume and muscle tone. Muscle tension is more pronounced in the early stages of the development of the pathological process.
2. Instability is not compensated by muscle tension. Displacement of the vertebrae leads to their subluxation, constant pain and arthrosis of the intervertebral joints.
The severity of compensation determines the condition of the patient with spinal instability. Disc fibrosis leads to an increase in its rigidity, a decrease in mobility in the spinal segment, a decrease in irritation of the nervous structures and a decrease in pain intensity. Instability that begins early in life may have a relatively worse prognosis than vertebral misalignment that develops in an older person. Over time, the mobility of the vertebrae decreases due to the development of fibrosis, spondylosis and spondyloarthrosis. As a result of these processes, people over 50 years of age experience a decrease in the frequency of neck pain compared to the younger population [8].
What diseases can have similar manifestations?
Very often, manifestations of “osteochondrosis” are actually associated with a completely different disease. For example, the cause may be hidden in the muscles - there is a condition called myofascial pain syndrome . Pain occurs due to constant tension in the same muscles.
Sometimes dizziness associated with otolithiasis, a condition in which crystals of calcium salts accumulate in the inner ear, is taken to be a manifestation of “cervical osteochondrosis.”
Each situation needs to be analyzed individually. A neurologist at the International Clinic Medica24 center will correctly assess your symptoms, prescribe the necessary examination, establish a reliable diagnosis and recommend effective treatment. Appointments can be made 24 hours a day by calling +7 (495) 230-00-01.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Pain and crunch in the neck, headaches - when these symptoms occur, many people “diagnose” themselves with osteochondrosis. Everything is clear - when it hurts, you need to take painkillers or get an injection, apply heat, and everything will go away. Why go to the doctor if you can handle it yourself?
However, self-medication often does not lead to anything good. Painful attacks may become more frequent, severe, and prolonged over time. If you uncontrollably take painkillers almost every day, you can get stomach or kidney problems. After all, any medicine has side effects.
And the cause of pain is not always due to osteochondrosis. In order to find out the real reason and understand how to effectively deal with it, you need to visit a doctor and undergo an examination.
Neurological manifestations of instability
With spinal instability, displacement of the vertebrae leads to a narrowing of the spinal canal, irritation of the dura mater, spinal cord and its roots, resulting in the development of neurological disorders, which are grouped into three groups of syndromes:
1. Radicular syndromes: lumbago, cervicalgia, radiculitis.
2. Neurodystrophic syndromes: anterior scalene muscle, pectoralis minor muscle, glenohumeral periarthritis, epicondylopathy, vertebral artery syndrome, cardiac syndrome.
3. Spinal syndromes: anterior horn syndrome, posterolateral syndrome, posterior column syndrome, conduction disorders.
Post-traumatic instability
Develops as a result of trauma, which includes fracture, fracture-dislocation and dislocation of the vertebrae. When the spine is damaged, flexion, flexion-rotation, extension and compression mechanisms of injury operate. The first two mechanisms operate in road and sports injuries and account for 70% of the total number of spinal injuries. The extensor mechanism occurs when the head is thrown back sharply and is found in whiplash-like motor vehicle injuries. The compression mechanism is associated with a sharp load along the axis of the spine and acts when falling from a height. Post-traumatic instability complicates about 10% of cases of vertebral fractures and fracture-dislocations. After an injury, the segment of the spine in which damage to either the anterior or posterior supporting complexes occurs is unstable. Post-traumatic instability produces spinal or radicular symptoms. In case of traumatic injury, displacement of the vertebrae by more than 3.5 mm and an increase in the angle between the endplates of adjacent vertebral bodies by more than 11° are interpreted as the result of gross damage to the ligamentous apparatus. According to A. White [2], damage to the posterior supporting complex with displacement of the vertebral body up to 2 mm and articular processes up to 1/3 can be considered a favorable variant of the course of instability. At the same time, complete destruction of the anterior supporting complex with displacement of the vertebral bodies of 2 mm or more is considered unfavorable in terms of prognosis. In such patients there is reason for the progression of instability.
Post-traumatic instability occurs in all age groups. In children, instability develops both as a result of intranatal trauma to the cervical spine during obstetric care, during which damage to the cervical spine ligaments occurs, and as a result of postnatal compression fractures of the vertebral bodies with unstable damage to the intervertebral discs and ligaments [4]. In adults, after a spinal injury, a decrease in the height of the intervertebral discs, pathological mobility and displacement of the vertebrae caused by disc damage and ligament rupture are found in the damaged area. In isolated vertebral fractures, which are not accompanied by ligament rupture and vertebral displacement, there is residual stability due to the preservation of the supporting complexes of the spine.
First aid
Of course, you should first do a spinal x-ray or other test to determine an accurate diagnosis. First, in case of severe pain, you can take a painkiller: “Tempalgin”, “Dolaren”, “Analgin”. If this group of drugs does not help relieve pain, you can take Ibufen, Diclofenac or Nise, but keep in mind that such drugs have a negative effect on the gastrointestinal tract. Therefore, this can only be an emergency, and then immediately consult a doctor.
You can also apply pain-relieving ointments. It is allowed to take diuretics if swelling appears in the area of inflammation. You can also use a Shants collar, but you should not wear it for a long time.
Degenerative instability
Degeneration of intervertebral discs occurs with spinal osteochondrosis. Degenerative-dystrophic changes consist in the disintegration of the fibrous ring and fragmentation of the disc tissue, which leads to a decrease in its fixation ability. Degeneration of the intervertebral disc can be either primary, due to a violation of cartilage metabolism, or secondary, due to a violation of the statics of the spine [7]. When a load is placed on a segment of the spine with a degenerated defective disc, pathological mobility and displacement of the vertebrae occurs, which is called degenerative spondylolisthesis or pseudospondylolisthesis. Displacement of the vertebra causes overload in the posterior supporting complex with the development of degenerative spondyloarthrosis. When the vertebrae are displaced, extensive changes develop in both supporting complexes, from where pain impulses come. In 85% of cases, instability with severe disc degeneration is observed at the CIII-CIV, CIV-CV and CV-CVI levels [2, 7].
Laboratory methods
To form a complete picture of the disease and clarify the diagnosis, to exclude other diseases with a similar clinical picture, the patient is prescribed an ECG (if necessary, with consultation with a cardiologist), blood tests, urine tests and other biological materials. The doctor identifies the level of calcium in the body, ESR, the patient’s immunity status and other indicators. They are important for differential diagnosis when it is necessary to distinguish between osteochondrosis and diseases of the internal organs.
In our clinic, doctors take an individual approach to examining each patient. They recommend tests and studies aimed at clarifying the condition of an individual patient.
The treatment is complex, including medications, physiotherapeutic methods, therapeutic massage, exercise therapy.
The rich experience of our specialists and the accuracy of the equipment will not make you doubt the diagnosis and successful treatment.
Postoperative instability
Postoperative spinal instability is associated with disruption of the integrity of supporting complexes during surgery. In practice, postoperative instability is most often observed after laminectomy, the extent of which has a significant impact on spinal stability. Unilateral laminectomy is a relatively gentle operation, while bilateral laminectomy with resection of the articular facets significantly worsens the support ability of the spine. A decrease in the load-bearing capacity of the posterior supporting complex leads to a redistribution of the load in the spine, resulting in an increased load on the vertebral bodies and intervertebral discs, which contributes to the further progression of their degeneration after a significant period of time after the intervention. The development and progression of postoperative spinal instability is associated with the influence of several factors:
1) inadequate load on the spine in the postoperative period;
2) ongoing disc degeneration and recurrent hernia;
3) errors and shortcomings in surgical technique in the form of an unreasonably large volume of resection of bone and ligamentous structures and lack of fixation of the spine;
4) development of instability at a level adjacent to the level of surgery. Spinal fusion after laminectomy can lead to overload of segments ranging from 60 to 180% [7], which are located above and below the level of spinal fixation.
To eliminate postoperative instability, repeated operations are required, which are not inferior in complexity to the primary intervention.
Dysplastic instability
Dysplastic instability of the spine develops due to dysplastic syndrome. Signs of dysplasia are found in the vertebral body, intervertebral disc, intervertebral joints and spinal ligaments.
Instability at the lower cervical level is associated with congenital inferiority of the intervertebral disc. A manifestation of dysplasia is the eccentric position of the nucleus pulposus, narrowing of the intervertebral disc, disruption of the integrity and parallelism of the endplates, as well as wedge-shaped vertebral bodies. In dysplasia, a change in the structure of collagen fibers leads to disruption of the hydration process of the tissue of the nucleus pulposus, which causes a violation of the mechanical properties of the intervertebral disc, a decrease in the rigidity of fixation of the vertebrae, and a violation of the relationship between the nucleus pulposus and the fibrous ring. These changes lead to the development of spinal instability at levels from CI to CII [5, 9].
In the atlantoaxial region, signs of dysplasia are found in the vertebral bodies, intervertebral joints and the entire ligamentous complex. Patients with craniovertebral pathology have a number of characteristic radiographic changes: asymmetry and inclined position of the odontoid process of the CI vertebra, hypoplasia of the atlas and condyles of the occipital bone, asymmetry of the atlantoaxial and atlantooccipital joints, asymmetry of the lateral masses of the atlas, synostosis of the CI and CII vertebrae, basilar impression and platybasia, rotation and flexion-extension instability of the spine [6]. Craniovertebral pathology is accompanied by multiple signs of dysplastic development in the form of a high hard palate, malocclusion, asymmetry of the face and shoulder girdle, shoulder blades, waist triangles, as well as flat feet, dysplastic instability of the shoulder, elbow, metacarpophalangeal and knee joints. Congenital inferiority of the ligamentous apparatus in the craniovertebral region leads to the development of decompensated instability.
With congenital concrescence of the CI and CII vertebrae, as well as with assimilation of the atlas, restriction of movement occurs at the upper cervical level with a decrease in the amplitude of movements, which leads to compensatory development of hypermobility in the lower cervical spine. The increased load creates conditions for rapid wear of the intervertebral discs and the development of instability at the CIV-CV and CV-CVI levels.
Dysplastic changes can affect any element of the spine. Congenital underdevelopment of the bursa-ligamentous apparatus forms the syndrome of the posterior support complex, described by A.V. Demchenko in adolescents [9]. Dysplastic changes lead to the early development of a degenerative process at a young age with impaired spinal stability. Congenital asymmetry of intervertebral joints, or tropism, manifests itself in changes in the size and position of the articular facets. Changes in the plane of the intervertebral joints cause changes in the rigidity of the posterior supporting complex, redistribution of the load on both supporting complexes, and early degeneration of the spinal segment, which is complicated by its instability. Underdevelopment of the articular processes leads to overstretching of the joint capsule, displacement of the articular surfaces, narrowing of the intervertebral foramina, looseness of the intervertebral joints, a decrease in the rigidity of the posterior supporting complex and an increase in the load on the anterior supporting complex. Disproportionately large articular processes lead to increased rigidity of the posterior supporting complex, which contributes to an increase in the load on this part of the spine.
In adulthood, dysplasia of the intervertebral joints is the cause of the development of dysplastic osteochondrosis, which can lead to both spinal instability and spondyloarthrosis.
Treatment of symptoms of cervical osteochondrosis
It is better not to self-medicate. Even if you have proven methods that usually help cope with pain, this does not mean that you are doing everything right.
Pain can be caused not only by osteochondrosis, but also by intervertebral hernia, muscle disorders (myofascial pain syndrome), and be a symptom of other diseases. In order to properly treat the disease, you need to understand its causes and carry out differential diagnosis. This is only possible in a clinical setting.
In order to identify the cause of the disease and properly treat the symptoms of cervical osteochondrosis, you need to visit a neurologist and undergo an examination.
Visit a specialist doctor at the Medical Center International Clinic Medica24. Make an appointment by phone at any time of the day: +7 (495) 230-00-01.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Cervical osteochondrosis is based on damage to the intervertebral discs. Their chemical composition is disrupted, first they swell, then decrease in size, cracks and tears appear in their outer part, and they become denser. Then the degenerative process spreads to the vertebrae and intervertebral joints. By reducing the height of the intervertebral disc, the load on the vertebrae increases, and bone growths – osteophytes – appear on them.
Conservative treatment
Conservative treatment is based on the controlled process of fibrosis of the intervertebral disc in an unstable segment of the spine. Wearing a head support promotes the development of disc fibrosis and stops the progressive displacement of the vertebrae. In an adult patient, the development of fibrosis can lead to gradual relief from pain. As a rule, treatment of spinal instability begins with the use of conservative methods. Conservative treatment methods are indicated in patients with instability of minor severity, which is not accompanied by severe pain and spinal symptoms. Conservative treatment methods include the following:
1) adherence to a gentle regimen;
2) wearing a soft or hard head holder;
3) taking non-steroidal anti-inflammatory drugs (NSAIDs);
4) novocaine blockades for exacerbation of pain syndrome;
5) massage and physical therapy of the back muscles;
6) physiotherapy (electrophoresis, ultrasound).
How does a neurologist diagnose cervical osteochondrosis? What happens in the doctor's office during an examination?
During your first appointment, the neurologist will ask you some questions:
- How long have you been bothered by headaches or neck pain?
- Where does the pain occur? What is their nature: stabbing, aching, shooting, pulling?
- When does pain usually occur? What triggers it? After what do you feel better?
- Have you already visited a doctor? Have you been examined and treated? Which? How long ago?
- What other symptoms bother you?
- What other chronic diseases do you have?
- Have you recently had a neck injury?
The doctor will then perform a neurological examination, checking your reflexes, skin sensitivity, and muscle strength and tone. You will be asked to turn, tilt your head to the sides, forward, backward. The doctor will press lightly on your head and on certain points in the neck to determine the occurrence of pain.
After the examination, you will be diagnosed and prescribed the necessary diagnostic methods.
The medical center International Clinic Medica24 employs experienced neurologists and uses the most modern diagnostic methods. You will be quickly and reliably diagnosed and prescribed effective treatment methods.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly