Indications for testing and symptoms of sinusitis
The main symptoms that may prompt a doctor to examine the frontal sinuses to make a diagnosis are:
- difficult and sometimes almost impossible nasal breathing;
- purulent and profuse nasal discharge;
- swelling and redness of the eyes;
- headaches, dizziness;
- swelling, tension and pain when pressing on the soft tissues near the maxillary sinuses, in the forehead;
- nose bleed;
- fever, general deterioration of the patient’s well-being, weakness.
The difference between frontal sinusitis and sinusitis is the localization of inflammation. In case of sinusitis, the focus of inflammation is the maxillary sinuses, in case of frontal sinusitis - the frontal sinuses.

X-ray of the sinuses
Frontitis (inflammation of the mucous membrane of the frontal sinus)
is an inflammation of the mucous membrane of the frontal sinus. Inflammation occurs due to infection with pathogenic organisms such as viruses, bacteria, and fungi. As a result of inflammation, swelling and blockage of the frontal-nasal tract occurs with purulent contents, which accumulate in the sinus, burst its walls and put pressure on the nerve receptors, which leads to frontal sinusitis.
Symptoms
There are acute and chronic processes of frontal sinusitis.
An acute process occurs most often against the background of influenza, rhinitis, as well as during trauma due to swelling of the mucous membrane and blockage of the frontonasal canal. The acute process is characterized by:
- increase in body temperature to 38 degrees
- sharp pain in the forehead, eyes, with pressure the pain intensifies
- copious nasal discharge (serous or serous-purulent)
- nasal breathing is difficult.
Have you noticed the following symptoms? Make an appointment
If frontal sinusitis is treated incorrectly, or in its absence, the acute process can turn into chronic frontal sinusitis due to insufficient drainage of the frontal sinus.
The chronic process most often occurs when the nasal septum is deviated. With each cold, the risk of frontal sinusitis increases. Chronic frontal sinusitis is marked by more subtle symptoms than in the acute form:
- aching headache
- pain on the affected side of the sinus, worsens with pressure
- purulent nasal discharge with an unpleasant odor, which flows down the nasopharynx during sleep, and in the morning the patient expectors a large amount of sputum.
Causes of the disease
The reasons for the development of frontal sinusitis may be:
- the presence in the body of a chronic source of infection (caries, tonsillitis), bacterial carriage (staphylococcus, streptococcus)
- runny nose
- previous trauma to the nose and, as a consequence, circulatory disorders and swelling of the mucous membrane
- deviated nasal septum
- congenital anomalies of the nasal cavity
- adenoids and polyps - can block the canal between the nasal passage and the paranasal sinus
- past diseases - influenza, ARVI, scarlet fever, diphtheria, rhinitis, sinusitis, sinusitis
- decreased immunity
- chronic diseases of the upper respiratory tract
Diagnostics
After an examination by an ENT doctor, as a rule, an x-ray of the paranasal sinuses is prescribed; in some cases, an ultrasound examination of the frontal sinuses and computed tomography are indicated.
To determine sensitivity to antibiotics, it is necessary to take a general blood test and bacterial culture of nasal discharge.
We recommend that you consult a doctor! 276-00-15
To determine the source of infection, rhinoscopy (examination of the nasal cavity using an endoscopic method) is indicated, with the help of which a possible curvature of the nasal septum can be identified.
Treatment
Treatment of frontal sinusitis is carried out conservatively, in some cases surgical treatment is indicated (for purulent form).
In general, for the treatment of frontal sinusitis, the doctor prescribes vasoconstrictor drugs in the form of drops or sprays; if the process of frontal sinusitis is purulent, broad-spectrum antibiotics are prescribed. Once a tank culture is obtained, treatment may be adjusted depending on sensitivity to antibiotics.
If frontal sinusitis is caused by a viral infection, antiviral therapy is prescribed; for a fungal infection, antifungal drugs are prescribed. Additionally, immunomodulators are prescribed to support the immune system.
doctor
Depending on the severity of the process, rinsing of the paranasal sinuses by moving the fluid may be prescribed. In this case, the medicinal solution is injected into the nasal cavity, the solution passes through the paranasal and frontal sinuses, and comes out with a stream of liquid, washing out the purulent contents and mucus. But if treatment does not improve and the level of pus increases, surgical treatment of frontal sinusitis is indicated.
A modern and effective method of treating frontal sinusitis is the expansion of the frontonasal anastomosis using an endoscope, during which the pus drains abundantly. This procedure is not traumatic and does not maintain a cosmetic effect. The procedure is performed under local anesthesia.
Another method of treating sinusitis without a puncture is the use of the YAMIK sinus catheter, where, when different levels of pressure are created in the paranasal sinuses, pus flows out.
Which method of treating frontal sinusitis will be effective in a particular case can only be decided by a specialist based on the examination and the patient’s symptoms.
Possible complications
Frontitis can lead to intracranial complications: purulent meningitis, brain abscess, which can even cause death.
X-ray procedure of the sinuses and forehead
Immediately before the x-ray procedure, you need to remove all metal jewelry from the area under study, in this case, remove earrings, chains, metal hair clips, and elastic bands. The patient's chin is placed on a special stand, the mouth must be opened slightly and, at the radiologist's signal, the breath must be held. After 10 - 15 seconds the procedure will be completed.

X-ray procedure
Causes and course of the disease
This disease is based on a viral infection and childhood diseases such as measles, scarlet fever, rubella, etc. The causative agents of the disease are representatives of the coccal flora.
In adults, swelling of the mucous membrane of the nasal cavity spreads to the middle nasal passage, which causes difficulty in outflow and blockage of the anastomosis in the area of the middle nasal passage. Isolated inflammation is extremely rare; the neighboring sinuses are usually involved: the frontal and maxillary. The most common cause of acute ethmoiditis is a violation of the patency between the nasal cavity and the sinus anastomosis, a decrease in the body's reactivity. This disease is promoted by such anatomical features of the nose as hypertrophy (enlargement) of the nasal turbinates, curvature of the nasal septum, the presence of spines and ridges of the nasal septum, and the polypous process of the nasal cavity.
In children, the course of this disease is aggravated by the presence of adenoid vegetations (proliferation of lymphoid tissue in the area of the dome of the nasopharynx).
Decoding and diagnosis
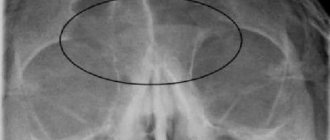
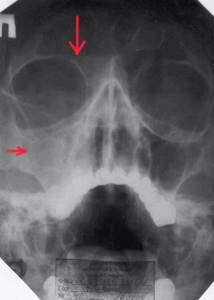
After receiving the image, the doctor will carefully examine it. If there is darkening of the frontal sinuses on an x-ray, frontal sinusitis can be diagnosed. In addition to darkening, the presence of exudative fluid will be visible in the image, this once again confirms the presence of an inflammatory process.
Osteoma of the frontal sinus on an x-ray can also cause darkening to be detected on an x-ray.
Darkening on an x-ray image
At the age of up to 18 years, due to physiological characteristics, underdevelopment of the frontal sinuses is detected on x-ray.
If any pathology is present, the radiologist refers the patient to a doctor specializing in the detected disease.
Magnetic resonance imaging (MRI) in St. Petersburg
Acute sinusitis is inflammation of the paranasal sinuses. Usually the process also involves the nasal mucosa, therefore, the process is correctly called rhinosinusitis.
Sinusitis is a common disease with a clear seasonal predisposition. The economic damage from disability and treatment costs runs into the billions.
Rhinosinusitis can be classified by anatomical region: sinusitis, frontal sinusitis, ethmoiditis and sphenoiditis; and by type of pathogen: bacterial, viral and fungal.
Acute sinusitis is a clinical diagnosis. It is fundamentally important to differentiate it from allergic and vasomotor rhinitis, as well as from a banal upper respiratory tract infection. Repeated episodes of acute sinusitis within a year at intervals of at least 8 weeks are considered a relapse. The duration of the process from 4 to 12 weeks allows us to talk about subacute sinusitis, more than 12 weeks already indicates a chronic process.
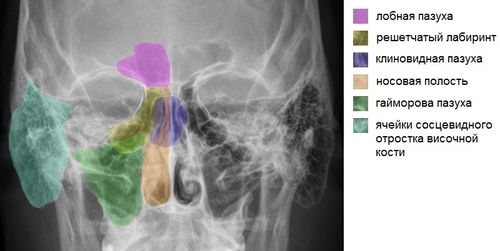
Anatomy and function
The paranasal sinuses are air-filled bony cavities that extend from the base of the skull to the alveolar process and laterally from the nasal cavity to the inferomedial margin of the orbit and the zygomatic process. The cavities of the sinuses are lined with villous epithelium, passing through the openings into the epithelium of the nasal cavity. The epithelium contains submucosal and seromucous glands that produce superficial mucus.
The anterior and posterior ethmoid sinuses consist of many air cells separated from each other by thin bony septa. Each cell is drained by an independent hole with a diameter of 1-2 mm, which is easily blocked by mucus or edematous mucosa. The main (sphenoid) sinus is located immediately behind the cells of the ethmoid bone and is bordered posteriorly by the sella turcica.
The arterial blood supply to the paranasal sinuses comes from the branches of the external and internal carotid arteries. Venous and lymphatic drainage goes into the plexus of the nasal cavity, as well as through valveless vessels directly into the arterial bed.
All sinus openings drain into the nasal cavity under the middle and superior turbinates through several anatomical structures united in the ostiomeatal complex. The openings of the maxillary sinuses, anterior cells, and frontal sinuses drain to a common location in the middle meatus. This place is called the lunate cleft, and is a narrow gap between the uncinate process and the large vesicle of the ethmoid bone. A single drainage site for the sinuses leads to relatively easy spread of infection even with local inflammation. The posterior cells and main sinus drain into the sphenoethmoidal recess located in the superior meatus below the superior turbinate.
The process of effective drainage consists of a complex interaction of the movements of the epithelial villi, the specific viscosity of the mucus and the diameter of the holes.
The function of the paranasal sinuses is diverse: reducing the weight of the skull, equalizing pressure, humidifying and warming inhaled air, absorbing heat and preventing overheating of the brain, sound resonance, increasing the olfactory area.

CT scan. The anterior ostiomeatal complex is normal. CT. Frontal plane. Designations: solid line – entrance to the ethmoid sinus, dotted line – cleft semilunaris, asterisk – opening of the maxillary sinus, 1 – middle meatus, 2 – uncinate process.

CT scan: Lunar cleft (frontal recess) is normal. CT. Frontal plane. Designations: 1 – frontal pocket, 2 – nasal cells.

CT scan. Sphenoethmoidal recess (posterior ostiomeatal complex). CT. Frontal plane. Designations: 1 – opening of the sphenoid sinus, 2 – pneumotized vomer.

CT scan. Anatomy of the sinuses. CT. Sagittal reconstruction. Designations: dotted lines upper - infundibulum of the ethmoid sinus, lower - lunar cleft, 1 - mucosa of the middle concha, 2 - mucosa of the inferior concha, 3 - frontal recess, 4 - opening of the sphenoid sinus, 5 - sphenoethmoidal recess, 6 - sphenoid sinus.
Pathophysiology
Thanks to the unidirectional (towards the nasal cavity) flow of mucosal secretion, the paranasal sinuses remain sterile. Swelling of the nasal mucosa at the site of drainage holes leads to stagnation of mucus and easy infection. With stagnation, secondary hypoxia of the villous epithelium develops and disruption of its function, as well as an increase in mucus viscosity. Dysfunction of the villous epithelium can also be genetically determined in Kartagener syndrome (situs inversus, chronic sinusitis and bronchiectasis), caused by the direct toxic effect of bacteria and viruses, as well as allergic diseases.
Anatomical factors may also contribute to outflow disturbances. The most common is the elongated uncinate process. This results in closure of the cleft semilunaris. The same is observed with lateral deviation of the apex of the uncinate process. Pneumotized turbinates of the middle meatus (concha bullosa) can compress the uncinate process and block the middle meatus. Haller's infraorbital air cells normally extend downward into the ethmoid bladder and the roof of the maxillary sinus. When large, they move into the cells of the ethmoid bone and compress the middle nasal meatus. The enlarged ethmoidal bladder (bulla) has the same functional significance. The curvature of the nasal septum and its spines, the paradoxical curvature of the turbinates, and the enlarged ethmoidal bladder contribute to the disruption of the outflow. Drainage failure may also be due to mechanical obstruction by a polyp, tumor, or foreign body.

CT scan. The uncinate process is elongated towards the bottom of the ethmoid bone. CT. Frontal plane. Designations: 1 - elongated uncinate process, 2 - concha bullosa of the middle concha, 3 - normal uncinate process, 4 - infundibulum of the ethmoid bone.

CT scan: Laterally deviated uncinate process. CT. Frontal plane. Designations: 1 - uncinate process deviated towards the orbit, 2 - normal uncinate process.

CT. Concha bullosa middle concha. CT. Frontal plane. Designations: 1 - the uncinate process reaches the bottom of the ethmoid sinus, 2 - the ethmoidal infundibulum is narrowed, 3 - concha bullosa, 4 - the uncinate process is absent on the right.

CT scan. Enlarged ethmoidal bladder (arrows).

CT. Concha bullosa middle concha. CT. Frontal plane. Designations: 1 - the uncinate process reaches the bottom of the ethmoid sinus, 2 - the ethmoidal infundibulum is narrowed, 3 - concha bullosa, 4 - the uncinate process is absent on the right.

CT. Paradoxical curvature of the middle concha with narrowing of the nasal passages.
Etiology
In the vast majority of cases, acute rhinosinusitis is caused by a viral infection: rhinovirus, less commonly, coronavirus, influenza and parainfluenza viruses, syncytial virus of the upper respiratory tract, adenovirus and even enterovirus. In 0.5-2% of cases, viral sinusitis is accompanied by a bacterial infection. Bacterial sinusitis can be caused by one or more pathogens, such as staphylococci (S. aureus), streptococci (S. pneumoniae, S. pyogenes), pneumococci (H. influenza), as well as other flora (P. aeruginosa M. catarrhalis, E coli, P. mirabilis, K. pneumoniae, Enterobacter). Fungal sinusitis is very rare. The direct pathogens are Aspergillus and Alternaria; other types of fungi can cause allergic sinusitis.
Clinical manifestations
Manifestations of the disease are nonspecific, usually against the background of a typical upper respiratory tract infection:
- Pain in the face, especially the forehead. Often the pain intensifies when bending over. They can radiate to the temporal and occipital regions.
- Redness and swelling of the skin of the nose, cheeks, hyperemia of the eyeballs
- Poor nasal breathing and nasal discharge
Symptoms of a viral infection lasting longer than 2 weeks are a warning sign for sinusitis. Acute viral sinusitis usually heals spontaneously, however, in about 1 out of 3 cases, acute sinusitis becomes chronic. A local complication of sinusitis can be a mucocele. It is an epithelial cyst that occurs as a result of obstruction of the duct of the secreting gland or the opening of the sinus. Cysts of the maxillary sinuses are often an incidental finding during X-ray examination. They reach large sizes and are usually asymptomatic. In contrast, cysts of the frontal and sphenoid sinuses cause clinical symptoms and are sometimes complicated by bone erosion.
Worsening of clinical symptoms is suspicious for a bacterial infection. In rare cases, bacterial sinusitis can lead to severe complications - toxic shock, meningitis and encephalitis, osteomyelitis.
Radiography
Radiography, despite its significant shortcomings, remains the most widely used research method for sinusitis. The study is desirable in 3 projections: occipitomental, occipitofrontal and lateral.
In the occipitomental projection, the maxillary sinuses are most clearly visible. The frontal sinus is visible in the oblique plane. The main sinus can be traced through the open mouth. The cells of the ethmoid bone are the worst visible.
In the occipitofrontal projection, the frontal sinuses and the bottom of the maxillary sinuses, as well as the anterior cells of the ethmoid bone, are best visible. The main sinus is less visible.
In the lateral projection, the main and frontal sinuses are best visible, while the structures of the other sinuses are layered.
The most common finding in acute sinusitis is the fluid level. In chronic processes, thickening of the mucosa, retention cysts and shell hypertrophy are observed.
The main problem is the layering of structures and a large number of false results. In addition, it is impossible to assess the ostiomeatal complex and the condition of the posterior cells of the ethmoid bone. Complete shadowing of the sinus can be caused by either fluid or thickened mucosa. At the age of up to 3 years, the sinuses are not yet pneumotized, so standard radiography is not informative.
Fluid level (arrow) in the maxillary sinus. X-ray in lateral projection.

Polypous sinusitis in the right maxillary sinus and a retention cyst in the left. X-ray in the frontal (occipito-frontal) projection.
Computed X-ray tomography (CT)
is the method of choice for chronic sinusitis, as it makes it possible to understand the anatomical prerequisites for the process. The main diagnostic plane for stepwise CT scans is coronal. Sections should be 2-3 mm thick and of high resolution. Reformed images have lower resolution and are therefore undesirable. However, they may become a necessary measure in the presence of artifacts from metal dental structures. Spiral CT allows slice thickness to be reduced to 1 mm, which improves the quality of reformatted images. When using spiral CT, there is no need for frontal placement.
In the bone window, the ostiomeatal complex is clearly visible, and in the soft tissue window, fluid, polyps, and the spread of the process beyond the sinuses, including to the orbit, infratemporal fossa and brain, are clearly visible.
The most typical finding in acute sinusitis is polypous mucosal thickening. Fluid may be detected in the sinus, and its filling may be complete or partial. Chronic sinusitis often involves cells of the ethmoid bone. In addition to the thickened mucosa, polyps and retention cysts are visible. Retention cysts (mucoceles) are most often observed in the frontal and maxillary sinuses.
The main disadvantage of CT is the difficulty in differentiating a tumor localized in the sinus from stagnant fluid.

Right-sided ethmoiditis (arrow). CT. Frontal plane.

Cyst (mucocele) of the frontal sinus. CT. Frontal plane.
Magnetic resonance imaging
MRI of the paranasal sinuses is especially important in diagnosing complications, especially the spread of infection into the cranial cavity.
The standard study involves coronal T1- and T2-dependent MRI images. Fat suppression is recommended but not required. The need for other projections and pulse sequences is dictated by the specific clinical situation. If a tumor is suspected, a contrast study is recommended.
Fluid, retention cysts, and edematous mucosa are hyperintense on T2-dependent MR images. T1-dependent MRI images sometimes provide clarity, as retention cysts may appear lighter due to increased protein content. The fluid, on the contrary, is usually darker than the inflamed mucosa.
The main disadvantage of MRI is poor visualization of the bony boundaries of the sinuses. In addition, there is a high rate of false positive results. A small hyperintense signal from the mucosa on T2-dependent tomograms in the absence of clinical symptoms is often observed in healthy individuals. Thus, for uncomplicated acute sinusitis, MRI is not a mandatory diagnostic procedure.

Ethmoiditis. MRI of the paranasal sinuses. Transverse plane (enlarged), T1-dependent MRI image.

MRI. Acute right-sided sinusitis. Coronal T2-weighted MRI,
MRI in St. Petersburg USA
Interpretation of the image of the maxillary sinuses
Darkening of the maxillary sinuses in the image may indicate the presence of pus and an inflammatory process in them; as a rule, the diagnosis in such cases is sinusitis. First of all, the ethmoid bone becomes inflamed, and if timely measures are not taken, the inflammation can spread to other bone tissues.

Maxillary sinuses
With less severe inflammation, the doctor may diagnose sinusitis.
In what cases are they referred for x-rays?
The patient is referred for an x-ray if the following symptoms and conditions are present:
- pain in the facial area;
- persistent nasal congestion;
- mechanical injuries and damage to the bones of the nose, facial and occipital skeleton;
- deviated nasal septum;
- suspicion of the presence of polyps, cysts and other neoplasms;
- adenoid vegetations in children and adolescents;
- foreign bodies trapped in the nasal passages;
- constant headaches of unknown etiology.
Most often, an x-ray of the sinuses is performed for sinusitis. Sinusitis is an inflammation that occurs in the paranasal sinuses and is accompanied by stagnation of mucous masses and pus. It can occur in one or several sinuses at once.
Let's figure out what sinuses are and how sinusitis manifests itself.
Contraindications to x-rays of the sinuses of the forehead and nose
As in most cases, radiography is contraindicated:
- during pregnancy and lactation;
- children under 15 years old.

If the patient's condition is serious, an x-ray may be prescribed, despite the presence of contraindications, using special protective pads. Before conducting a study, you must weigh all the risks and strictly follow the recommendations of your doctor.

You can take an x-ray of the sinuses of the forehead and nose in almost any medical institution, the only difference is that in government institutions the procedure is free, and in private the cost ranges from 1000 rubles.
Medical Internet conferences
According to numerous recent studies, in the structure of ENT morbidity indicators, one third is occupied by pathology of the paranasal sinuses (NS). Among the diseases of the sinuses, the first place belongs to the maxillary and ethmoid sinuses, and the frontal sinuses are affected somewhat less frequently, which can be explained by the more favorable anatomical location of the latter. However, the inflammatory process in them is much more severe, and quite often (from 0.8 to 3%) with severe intraorbital and intracranial complications, which is explained by the significant variability in the structure of the frontal sinuses (FS) and the variety of clinical manifestations of the pathological process in them. Inflammatory diseases of the LA, like all other SNPs, can cause damage to various internal organs, pathological conditions of the nervous system, allergization of the body, and changes in immunity. Individual anatomical features of the LA structure, significant dependence on the state of the structures of the nasal cavity (ostiomeatal complex, nasal septum, nasal turbinates, etc.), variability of subjective symptoms, difficulties in diagnostic examination and treatment process indicate the need to improve traditional and develop new diagnostic methods and methods LP diseases.
The anatomical proximity of such important organs as the brain, eyes, and the possibility of developing rhinosinusogenic complications especially emphasize the need for early diagnosis of sinusitis, predicting the very possibility of developing the disease and its prevention.
Before the introduction of computer tomograms into medical practice, the study of the anatomical structure of the paranasal sinuses, including the frontal ones, was carried out on cadaveric material, macerated turtles (V.P. Alekseev, G.F. Debets, 1964, M.V. Miloslavsky, 1903, V.S. Speransky, A.I. Zaichenko, 1980). Based on the above, the analyzed material in the form of existing collections of skulls is not numerous and limits the possibility of massive statistical research, including ethnographic differences in skulls, because do not contain a large number of skulls. Skulls undergo destruction over time, and to study the deeper structures of the skull, in particular the paranasal sinuses, its destruction is necessary. The advent of computed tomography solves all these problems.
Clinical picture
It is not much different from the clinical picture of acute sinusitis (maxillary sinusitis). Pain is localized in the area of the root of the nose and eye sockets. Palpation of the inner corner of the eye causes pain. During anterior rhinoscopy (instrumental examination of the nasal cavity), purulent discharge is noted not only under the middle turbinate, but also above it, since all the cells of the ethmoid bone become inflamed. There is a disturbance in nasal breathing and discharge from the nasal cavity, and hyposmia or anosmia (decreased or loss of smell) is common. The general condition noticeably worsens, there is malaise and an increase in body temperature, often to subfebrile levels.
Friends! Timely and correct treatment will ensure you a speedy recovery!
During an endoscopic examination of the nasal cavity, the mucous membrane looks very swollen and hyperemic (reddened). With a disease of the anterior cells of the ethmoid sinus, such changes and purulent discharge are observed in the area of the middle nasal passage, and in the case of the posterior cells, in the area of the upper nasal passage. This is due to the anatomical location of the anastomosis.
On examination, the middle turbinates are swollen and increased in size. After anemization (introduction of vasoconstrictors into the nasal cavity using a cotton probe), a strip of pus often becomes visible under the middle or superior turbinate. Isolated damage to the cells of the ethmoid sinus is rare; it is usually accompanied by inflammation of the frontal and maxillary sinuses, and then the sphenoid sinuses. When performing posterior rhinoscopy or endoscopic examination, changes are detected in the area of the sphenoethmoidal recess (upper parts of the nasal cavity).
In some cases, when the outflow of pus into the nasal cavity is difficult, the inflammatory process spreads to the orbital tissue, as a result of which pus can break into the orbit and damage its bone wall. This course of the disease is accompanied by a disturbance in the general condition, pain in the eye area, fever and headache.
Diagnostics
Diagnosis of acute ethmoiditis is based on identifying characteristic symptoms and data from studies.
Pain concentrated at the root of the nose and along its lateral surface, which correspond to the lower edge of the nasal bones and the frontal process of the upper jaw, may indicate damage to the anterior cells of the ethmoid labyrinth. X-rays, diaphanoscopy and computed tomography help clarify the diagnosis. Make an appointment right now!
Call us by phone or use the feedback form
Sign up
Treatment
Generally, conservative treatment is recommended, which is similar to the treatment of acute inflammation in other sinuses.
The dominant technique is still rinsing the paranasal sinuses by moving fluid because of its speed, convenience, and most importantly effect. If, after following the doctor's orders, there is no improvement within several days, hospitalization is necessary for surgical treatment - opening the cells of the ethmoid labyrinth. Endoscopic surgery is much preferable to classical ethmoidotomy, due to its higher quality and gentle (minimally invasive) approach.