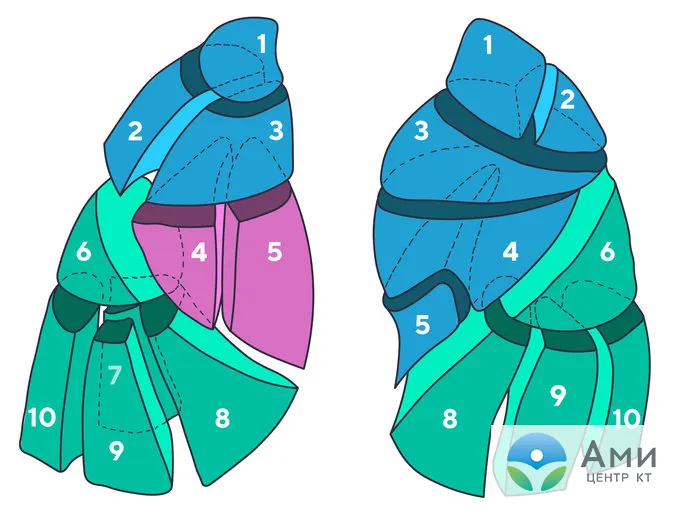
Lung segments (bronchopulmonary segments) are a conditional division of an internal organ into separate sections, accepted in medicine, necessary for a correct conclusion. According to a unified classification adopted at the International Congress of Anatomists in 1955 in Paris, the lungs consist of 19 segments - 10 in the right and 9 in the left. The segments are grouped into lobes: 3 in the right lung (upper, middle, lower) and 2 in the left lung (upper and lower).
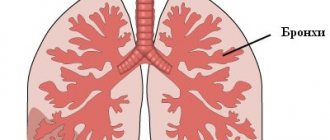
Each pulmonary segment includes part of the bronchial tree, arteries and veins, and is shaped like an irregular trapezoid, the smaller side of which is located closer to the roots and mediastinum, and the base is on the periphery, the outer side of the lungs.
The lung segments are divided in this way not arbitrarily, but anatomically. Segmental boundaries can be determined by interlobar fissures during surgery, internal boundaries can only be determined by their mechanical separation.
Lobes and segments of the lungs
Right lung
Upper lobe
Apical segment, S1 - located behind the second rib of the chest. Segment 1 of the lung includes airways with a total length of about 2 cm. The segment is connected by the airways to S2.
Posterior segment, S2 - in relation to the apical segment 2, it is located dorsally (lower, towards the back) at the level of 2-4 ribs. The segment is connected by the respiratory tract to S1, through the vascular branch to S3 and to the pulmonary artery.
Anterior segment, S3 - located frontally between the 2nd and 4th ribs. The 3rd segment of the lung includes the superior branch of the pulmonary artery.
It is with damage to the upper lobes of the lungs that most infectious and inflammatory diseases of the lungs begin, for example pneumonia, tuberculosis, granulomatosis. Since adjacent segments of the lungs, artery and bronchus are interconnected, it is important to promptly determine the type of infectious pathogen and begin treatment to prevent further spread of the disease.
Bullae (air cavities) in emphysema are also localized here.
Upper lobe
Lateral segment, S4 - located in the anterior part of the axilla between the 4th and 6th ribs.
Medial segment, S5 - located in the front of the chest at the level of the 4th and 6th ribs.
Thus, the 4th and 5th segments of the lung are located in the mid-frontal part of the lung at the same level, penetrated by tubular branches of the bronchi and vessels. At this level, neoplasms and metastases are found more often than in the upper lobes of the lungs.
Lower lobe
The upper segment, S6 - is projected onto the lower half of the scapula: from the center to the corner, at the level of 3-7 ribs. Blood supply in the 6th segment of the right lung is carried out through the artery - a continuation of the lower pulmonary.
The medial basal segment, S7, is also called the “cardiac” segment because it is located closer to the diaphragm on the inside, closer to the right atrium. A branch of the vena cava passes nearby. High-resolution computed tomography is the only research method in which the 7th segment of the lung is clearly visible.
Anterior basal segment, S8 - located at the level of the 6-8 rib in the projection from the middle of the axilla.
Lateral basal segment, S9 - located between the 7th and 9th ribs in projection to the posterior part of the axilla.
Posterior basal segment, S10 - located between the 7th and 10th ribs and adjacent to the spine.

Left lung
Upper lobe
The apical-posterior segment, S1-S2, is structurally and functionally practically no different from the 1st and 2nd segments of the right lung. The apical and posterior segments on the left side are often combined due to the common bronchus. Thus, this is the largest segment.
Anterior segment, S3 - located between the 2nd and 4th ribs closer to the sternum.
The upper lingular segment, S4, is located in the mid-anterior part of the chest at the level of 3-6 ribs in projection to the center of the armpit. This is also one of the largest segments.
The lower lingular segment, S5, is located under the 4th segment of the left lung. Separated from segment 4 by an interlobar fissure.
Lower lobe
The upper segment, S6 - in localization and structural and functional properties coincides with the 6th segment on the right.
Basal-medial, cardiac segment, S7 - in localization and structural and functional properties coincides with the 7th segment of the lung on the right.
Anterior basal segment, S8 - in localization and structural and functional properties coincides with the 8th segment of the lung on the right.
Lateral basal segment, S9 - in localization and structural and functional properties coincides with the 9th segment of the lung on the right.
Posterior basal segment, S10 - in localization and structural and functional properties coincides with the 9th segment of the lung on the right.
The sizes and shapes of the pulmonary segments depend on the individual characteristics of the patient’s body and may vary.
Many lung diseases, such as pneumonia, tuberculosis, and abscesses, begin with a small lesion in one segment of the lungs. According to their localization and specific pattern of the disease, which is visualized on tomograms.
By studying images on cross-sectional scans and 3D reconstructions, a radiologist can give an initial conclusion on the changes identified on a CT scan. Differential CT diagnostics means that in most cases the doctor will be able to accurately distinguish tuberculosis from pulmonary granulomatosis, and “ground glass” in pneumonia from tumor infiltrate.
Congenital lobar emphysema (CLE) is a developmental defect characterized by emphysematous stretching of the parenchyma of a lobe or segment of the lung due to impaired development of the cartilaginous structures of the bronchus of the affected lobe [1-10]. Other causes of lobar emphysema may be compression of the bronchus from the outside by cystic formations or abnormally located vessels, partial disruption of bronchial patency due to hyperplasia of the bronchial mucosa or mucus plugs [1-5].
The clinical picture of the disease was first described in detail in 1951 by R. Robertson, and E. Jazmes called it lobar emphysema [4, 5].
Based on radiological data and the severity of clinical manifestations, it is customary to distinguish between decompensated, subcompensated and compensated stages of the disease [2-5]. Subcompensated and decompensated stages occur in newborns and children in the first months of life; at these stages, intrathoracic tension syndrome is most pronounced. The compensated stage is observed in older children and is clinically similar to other lung diseases [4, 5].
At the compensated stage of VLE, clinical manifestations are very scarce. With a small degree of emphysematous expansion, the disease is often detected incidentally during an X-ray examination at an older age [5]. The incidence of VLE in children is 0.2% among acute lung diseases and 6.9% among lung malformations [3-5]. It has been noted that VLE in 65% of cases is combined with other developmental defects: segment hypoplasia, lung sequestration, arteriovenous aneurysm, developmental anomalies of the cardiovascular system, kidneys, intestines, and musculoskeletal system [3-5].
According to the literature, VLE is more common in the upper lobe of the left lung - in approximately 60% of cases. However, it is often localized in the upper or middle lobe of the right lung, and cases of its detection in the lower lobe are quite rare.
We observed a child with lobar emphysema of the lower lobe of the left lung.
Sick T.
, 13 years old, was admitted to the pediatric department of thoracoabdominal surgery of the National Medical Center of the Republic of Tajikistan on December 10, 2013 with a presumptive diagnosis of a foreign body in the respiratory tract. From the anamnesis it turned out that the child had been ill since birth and had been receiving outpatient treatment for a long time in various medical institutions for chronic pneumonia. During the next X-ray of the chest organs, a foreign body in the respiratory tract was suspected.
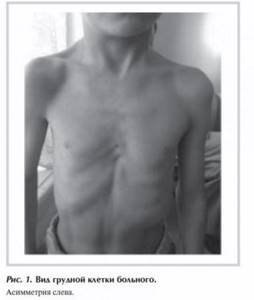
Upon admission, the patient's condition was satisfactory. When examining the chest, asymmetry of the chest is noted in the form of a bulge on the left with an increase in the intercostal spaces (Fig. 1)
.
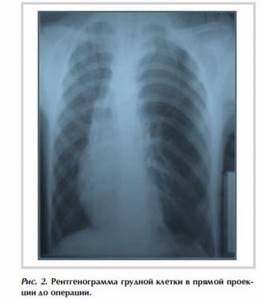
On auscultation, vesicular breathing is heard over the right lung, and weakened breathing is heard on the left along the anterior and posterior surface of the chest. The blood and urine test results correspond to the age norm. An X-ray of the chest organs in the projection of the upper lobe of the left lung shows increased airiness of the pulmonary fields, a pronounced depletion of the pulmonary pattern, displacement of the mediastinal organs to the opposite side, flattening and low standing of the dome of the diaphragm on the affected side (Fig. 2)
.
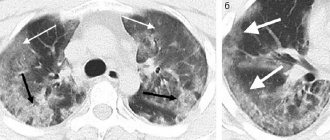
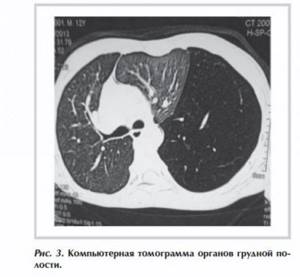
A computed tomography scan of the chest revealed signs of lobar emphysema of the upper lobe of the left lung.
A symptom of intrathoracic tension with a displacement of the mediastinal organs to the right is determined (Fig. 3)
.
A diagnosis was made: congenital lobar emphysema of the upper lobe of the left lung.
The operation was performed as planned on December 17. After thoracotomy on the left, it was discovered that the upper lobe was collapsed and displaced towards the mediastinal pleura, the lower lobe was emphysematously dilated, did not collapse during exhalation and occupied the entire pleural cavity. The interlobar fissure is well expressed. The vessels of the lower lobe were isolated, stitched and ligated. The bronchus of the lower lobe is divided and sutured. The share has been removed. The upper lobe of the lung is expanded. The pleural cavity is washed and drained.
A morphological study of the specimen revealed emphysematous changes in the lower lobe.
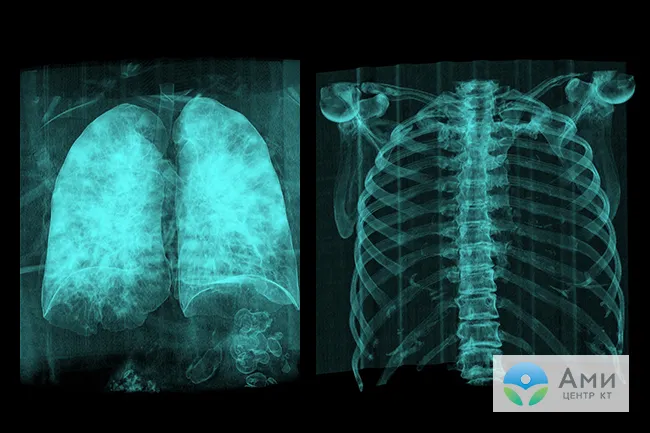
The pleural drainage was removed on the 6th day after surgery, after which hemothorax occurred (Fig. 4, a)
.

The complication was eliminated using pleural puncture.
Hemostatic and symptomatic therapy was carried out. On radiography, the left pulmonary field is reduced in volume and pneumatized. Focal shadows are not detected. The roots of the lungs are structural. The mediastinal shadow is not expanded. Sinuses are free (see Fig. 4, b)
.
The patient was discharged in satisfactory condition on the 16th day after surgery.
The difficulty of diagnosing VLE is associated with the paucity and nonspecificity of the clinical manifestations of the disease.
In our case, VLE of the lower lobe of the left lung was an intraoperative finding. Based on the examination data of this patient (X-ray and CT of the chest organs), the presence of VLE in the upper lobe of the left lung was assumed. The difficulty of diagnosing such a disease is determined by the rarity of the developmental defect.
What does a CT scan of the lungs show?
Studies show that the lobes of the lungs, like segments, are not reliably determined on an x-ray, even if it is a digital device, and the study was carried out with additional contrast enhancement of the images.
CT scan of the lungs allows you to examine the organ “from the inside,” sequentially viewing scans of each section (step size up to 1 mm) in high resolution. In this way, the radiologist can determine the boundaries of the lobes and correctly formulate a conclusion for the attending physician - a pulmonologist, therapist or ENT specialist, who has the final say in making a diagnosis and prescribing therapy.
Computed tomography (CT, MSCT) of the lungs shows:
- Segmental structure of the respiratory organ and the slightest pathological changes;
- Integrity and patency of the respiratory tract;
- Condition of interstitial septa, inflammatory process;
- Impaired blood flow, thrombosis, vascular stenosis (CT with contrast);
- Enlarged lymph nodes;
- Foci of infectious and inflammatory process;
- Tumors;
- Metastases;
- Mechanical damage.
As part of the algorithm for examining the lungs on CT, the radiologist evaluates the anatomical components:
- Soft fabrics;
- Bone tissue;
- Diaphragm and sinuses;
- Roots of the lungs;
- Bronchial tree;
- Mediastinal organs;
- Interstitium and the architecture of the pulmonary matrix.