Breathing is a process without which a person cannot exist. Anyone who cares about their health should know where a person’s lungs are, how they function and what structure they have. The organ is vital because it supplies the entire body with oxygen.
Human lungs: brief characteristics of the organ
The functioning of the brain, the release of energy, and the breakdown of useful substances with the help of oxygen directly depend on the functioning of the respiratory system. The respiratory organs include the nose, mouth, larynx, trachea, and bronchi, which are part of the lungs.
The lung is one of the paired, most voluminous human organs. In a healthy state, it is pink-red in color, the structure is soft, spongy.
The average volume of the organ is 3 liters, but 450-500 ml is enough for inhalation and exhalation. In people who are actively involved in swimming, the lung volume reaches 5 liters.
For a deep breath, about two liters of atmospheric air are used. With such breathing patterns, a reserve remains in the organ, thanks to which the level of oxygen in the alveoli is maintained at the required level.
In the tissues of each lung, venous and arterial blood constantly moves, and lymphatic vessels are present. It also contains nerve cells that are closely connected with blood vessels and bronchi.
In the first month of pregnancy, the rudiments of the main organ of the respiratory system are already formed in the fetus, and by the fifth month its constituent elements are designated. The organ continues to grow until the age of 25, as the growing organism constantly needs oxygen.
Visibility on X-ray
On an x-ray, normal lung parenchyma is visible as homogeneous tissue, although in life this is not the case. The presence of extraneous lightening or darkening will indicate the presence of pathology. Using the X-ray method, it is not difficult to detect pneumonia, lung injuries, the presence of fluid or air in the pleural cavity, as well as neoplasms.
Cleared areas appear as dark spots on an x-ray due to the way the image is developed. Their appearance means increased airiness of the lungs with emphysema, as well as tuberculous cavities and abscesses.
Darkening zones are visible as white spots or general darkening in the presence of fluid or blood in the lung cavity, as well as in the presence of a large number of small foci of infection. This is what dense neoplasms, places of inflammation, and foreign bodies in the lung look like.
Lung segments and lobes, as well as medium and small bronchi, alveoli are not visible on the x-ray. Computed tomography is used to identify the pathologies of these formations.
Lung location
The lungs are located in the middle of the chest. They are protected and supported by a frame of ribs, 12 on the left and right. On the back side, the organs are protected by the spinal column.
To ensure the ability to breathe, there is muscle tissue between the ribs; the bones are fixed to the sternum by cartilage. From the back, the lungs are located 2-3 cm above the collarbones.
From below, the organ borders the diaphragm, which separates the peritoneum and chest. On the right side, under the lung, is the liver. On the left side, the heart is adjacent on top, and partly the stomach is below. The exact location of a person’s lungs can be clearly seen in the photo.
Applications of computed tomography
Computed tomography (CT) is one of the most accurate and modern research methods for any pathological process. The procedure allows you to view each lobe and segment of the lung for the presence of an inflammatory process, as well as evaluate its nature. When conducting research you can see:
- segmental structure and possible damage,
- change of share plots,
- airways of any size,
- intersegmental partitions,
- circulatory disorders in the vessels of the parenchyma,
- changes in lymph nodes or their displacement.
Computed tomography allows you to measure the thickness of the airways to determine the presence of changes in them, the size of the lymph nodes and view each section of tissue. The images are interpreted by a pulmonologist who makes a final diagnosis for the patient.
What is the structure of the human lungs?
The organs are similar in shape to half-cones, but are not identical in shape and size. The lung, located on the right, is shorter and wider than the left, and also larger. This is explained by the fact that the liver is located on the right. In the lung, located on the left, there is an inset for the fit of the heart. The organ located on the right has three lobes: lower, middle and upper. The left has only two lobes: upper and lower. Each lobe has segments that are supplied by a large blood and respiratory vessel.
Each lung contains:
- root, consisting of a vein, pulmonary artery and large bronchus;
- entrance gates, that is, small depressions through which the root passes into the lung and branches into smaller vessels and bronchi.
The segments of the bronchi and blood vessels are separated by layers of connective tissue and are shaped like pyramids. When studying the structure of the human lungs, it is important to understand that the organ has three main structural elements on which the ability to perform the respiratory function depends. This:
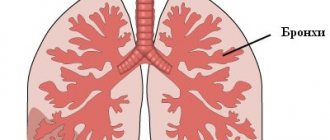
- Bronchi. They look like a forked tree trunk with numerous branches. They are located inside the lungs and are a continuation of the trachea, which is divided into two wide tubes, and then into 5 more branches: three in the right lung, two in the left. With each branching, the bronchi decrease in diameter.
- Alveoli. These are pulmonary vesicles whose purpose is gas exchange. They have thin walls and microscopic size. The inside of the alveoli is lined with surfactant, which prevents the membranes from sticking together. When you breathe through them, oxygen molecules penetrate into the blood, and then, with red blood cells, are carried through the circulatory system to all organs.
- Bronchioles. Formed at the ends of the bronchial branches. There are respiratory and terminal ones. At their ends are acini (the smallest parts of the bronchial tree).
Each lung is protected from the outside by the pleura. This is a special two-layer membrane that lies between the lung tissue and the sternum. The pleura contains biological fluid.
The structure also contains stroma - this is the internal framework of organs, thin connective tissue that divides the lungs into lobules. Inside the stroma there are blood and lymphatic vessels, nerve fibers, and air entry/exit pathways.
Features of the structure of the right lung
On the right, the organ is divided into three lobes according to their location.
Upper lobe part
S1 - apical, the front part is located behind the II rib, then to the end of the scapula through the pulmonary apex. It has four borders: two on the outside and two on the edge (with S2 and S3). The composition includes part of the respiratory tract up to 2 centimeters in length, in most cases they are shared with S2.
S2 - posterior, passes behind from the angle of the scapula from above to the middle. Localized dorsal to the apical one, it contains five boundaries: with S1 and S6 on the inside, with S1, S3 and S6 on the outside. The airways are localized between the segmental vessels. In this case, the vein is connected to that of S3 and flows into the pulmonary vein. The projection of this segment of the lungs is located at the level of the II–IV rib.
Lateral division
This segment is projected from the side of the medial part only as a narrow strip lying above the interlobar oblique groove. The bronchus has a posterior orientation. In this regard, the segment is located on the back part in the middle lobe. It is visible from the surface of the ribs. There are five boundaries in the department. Two of them lie along the medial surface, separating the anterior and medial segments of the lung. The first boundary lies in accordance with the terminal portion of the oblique groove. The other three are located on the costal surface of the organ. They separate the medial and lateral segments of the middle lung.
The first boundary runs vertically. It runs from the center of the horizontal furrow to the edge of the oblique. The second border runs between the anterior and lateral segments. It corresponds to the location of the horizontal groove. The third border is in contact with the posterior and anterior segments in the lower lobe. The vein, artery and bronchus are deep. The approach to them is only possible below the gate along an oblique furrow. The lateral segment is located in the area between the IV-VI ribs.
Existing classification
The most famous classification was adopted in London in 1949 and confirmed and expanded at the 1955 International Congress. According to it, in the right lung it is customary to distinguish ten bronchopulmonary segments:
In the upper lobe there are three (S1–3):
- apical;
- rear;
- front.
In the middle part there are two (S4–5):
- lateral;
- medial.
Five are found at the bottom (S6–10):
- upper;
- cardiac/mediabasal;
- anterobasal;
- laterobasal;
- posterobasal.
On the other side of the body, ten bronchopulmonary segments are also found:
The upper lobe includes five (S1–5):
- apical;
- rear;
- front;
- upper reed;
- lower reed.
In the part below, there are also five (S6–10):
- upper;
- mediabasal/inconsistent;
- anterobasal;
- lateralobasal or laterobasal;
- posterobasal/peripheral.
The middle lobe is not defined on the left side of the body. This classification of lung segments fully reflects the existing anatomical and physiological picture. It is used by practitioners around the world.

Anterior basal section
This segment is located in the lower lobe, its anterior section. On the sternum, its location corresponds to the VI-VIII ribs of the axillary midline. There are three boundaries in the department. The first line runs between the lateral and anterior segments in the middle lobe. It corresponds to the oblique groove. The projection of the second border coincides on the medial surface with the beginning of the ligament. The third line runs between the upper and anterior segments. The artery begins from the inferior branch of the common arterial canal. The bronchus arises from the process of the lower lobe element of the same name. The vein enters the inferior main venous branch. The bronchus and artery are visible at the bottom of the oblique groove under the visceral pleura. A vein is found under the ligament.

Contraindications
For non-small cell lung cancer, segmentectomy is often not enough to remove all the tumor tissue. The most common type of surgery for this cancer is removal of a lobe of an organ, a lobectomy. In some cases, the entire lung has to be removed (pneumonectomy).
At the same time, if the patient has severely impaired respiratory function, and there is no necessary reserve in the lung tissue, or there are severe concomitant diseases, then even segmentectomy may be contraindicated.
Other contraindications to this surgical intervention:
- Bleeding disorders - during surgery and in the postoperative period, this can lead to severe bleeding, which can be life-threatening.
- Infectious processes on the skin in the area of the intended incision or puncture site. In this case, the infection can be introduced into the chest cavity, and this will lead to serious consequences.
- Diffuse lung diseases, in which most of the lung tissue is affected.
- Malignant tumors with metastases. In this case, surgery will not help get rid of all the tumor tissue and is unlikely to be beneficial for the patient.
Make an appointment with a doctor at the Medica24 international clinic: he will assess your condition, tell you whether surgery is indicated in your case, and select the optimal type of surgical intervention.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Preparing for surgery
A preliminary examination is carried out, which helps to establish an accurate diagnosis and plan surgical treatment. The doctor consults the patient, talks about what type of operation is planned to be performed, why it is needed, and what the risks are. In turn, the patient must provide the doctor with information about what concomitant diseases he suffers from, what medications he takes, whether he has allergic reactions to medications and latex, and whether he suffers from bad habits (smoking, frequent drinking of alcohol).
If the patient is taking anticoagulants (drugs that reduce blood clotting), they may need to be stopped for a while.
It is recommended to stop smoking at least 30 days before surgery. This will help improve the functioning of the cardiovascular system, tissue healing, and reduce the risk of complications.
Before surgery, you need to undergo a preoperative examination. The doctor will give you a list of necessary studies and tests. It includes blood and urine tests, blood coagulation tests, ABO group, Rh factor, tests for HIV, syphilis, viral hepatitis, ECG, consultation with a therapist, etc.
Lung segmentectomy is performed under general anesthesia (anesthesia), so you should not eat or drink anything 10–12 hours before the operation.

Recovery period
After a segmentectomy, the patient may be admitted to the intensive care unit, where he will spend one night. Extubation (removal of the tube from the trachea) is usually possible in the operating room after the procedure is completed. The drainage tubes are checked every 8 hours. The next day, a blood test is performed to assess hemoglobin levels and kidney function. In the first 48 hours, the state of the cardiovascular system is monitored. Many patients experience pain in the postoperative period and require adequate pain relief. Since many patients undergoing lung surgery are smokers, they require oxygen therapy in the postoperative period.
The patient is discharged home after the drainage tubes are removed, he begins to ambulate independently and is placed on a semi-solid diet. In some cases, if air is released from the pleural space, the patient may be discharged with drainage tubes, and these will be removed after some time.
Typically, hospitalization time after open segmentectomy is 5-7 days, and after VATS - 2-3 days.
The following recommendations must be followed:
- For a speedy recovery and prevention of complications, breathing exercises and physiotherapeutic procedures are performed.
- You should avoid physical activity and driving for a week.
- It is necessary to adhere to the diet recommended by the doctor and come to the clinic for follow-up examinations on time.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Medial department
It is visible on both the medial and costal surfaces in the middle lobe. There are four boundaries in the department. Two separate the medial section from the lateral in the lower and anterior in the upper lobes. The second border coincides with the oblique groove. The first one runs along the front part of the horizontal recess. There are also two boundaries along the costal surface. One starts from the middle of the anterior zone of the horizontal furrow, descending to the final section of the oblique. The second boundary separates the anterior segment from the medial segment. The line coincides with the location of the horizontal groove. A segmental branch arises from the inferior branch of the artery. Below it there is a bronchus and a centimeter vein. The segmental pedicle is approached from the lower part of the hilum through the interlobar oblique groove. The border on the chest is located in the region of the IV-VI ribs along the axillary midline.

Manifestations of exophytic central lung cancer
Gradually closing the lumen of the bronchus, the tumor node causes its narrowing, as well as constant irritation and subsequent destruction of the mucous membrane.
This is accompanied by the appearance of a cough, the nature of which changes as the process progresses: dry ⇒ with an abundance of light sputum, sometimes mixed with streaks of blood ⇒ with purulent sputum.
An increase in the tumor leads to deterioration in ventilation of the affected lung, which ends in its collapse (atelectasis). Against the background of these changes, a special form of inflammation develops (cancerous pneumonia) with shortness of breath, fever, weakness, and a general deterioration in well-being. If the inflammation affects the outer lining of the organ (pleura), pain is added to the symptoms described above.