- Home /
- Branches /
- CT scan /
- CT coronary angiography (heart vessels)
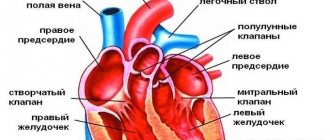
Multislice computed tomography (MSCT)
or coronary angiography of the arteries allows you to determine the presence of pathologies in the structure and functioning of the heart. It is considered the leading method for examining the cardiovascular system (CVS). It is a visualization method that produces a three-dimensional image. The heart and arteries can be examined layer by layer, which provides maximum information when identifying abnormalities.
To carry out the procedure, a contrast agent is injected into the ulnar or other peripheral vein. Unlike standard coronary angiography of the heart using contrast, this method allows you to track the condition of the coronary artery wall and the structure of plaques leading to stenosis.
What exactly does CT coronary angiography show?
The essence of coronary angiography is to assess the condition of the atria and ventricles, myocardial thickness, and view large arteries. The condition of the vascular bed, cardiac cavities and pericardium is examined, and valve pathologies are identified. In addition, the method is used to monitor the organ after bypass surgery.
Advantages
No special or lengthy preparation is required for the procedure. It is carried out with minimal introduction into the body and is safe, unlike many other methods.
After the examination, the doctor is left with a high-quality display of all the vessels and tissues of the heart, and their informative 3D model. This allows you to view structures layer by layer. It is best to perform coronary angiography of blood vessels in Moscow. The procedure itself is easy and quick for the patient. It takes 40-60 minutes and does not require difficult steps.
After coronary angiography
After the examination, the doctor will remove the catheter, use a stapler to close the blood vessel, or simply tape the needle site in the arm, groin or neck. Sometimes, after the catheter is inserted, a bruise or painful sensation may remain.
After a CT coronary angiography, you will remain under observation for some time in a medical facility. You will need to limit your movements to prevent bleeding from the hole where the catheter was inserted.
How is coronary angiography done?
The reason for this diagnosis may be unexplained pain in the chest area and suspicion of pathology in the development of blood vessels carrying oxygenated blood. It is also done before planned operations (bypass surgery), after them (assessment of the result) or to determine the patency of the arteries in case of stenosis.
Necessary preparation
Before the procedure, a coronary calcium index must be determined to assess the appropriateness of an examination with the introduction of a contrast agent. After this, blood is donated for biochemistry. The doctor is primarily interested in the level of creatinine and urea. If the patient has previously undergone ultrasound, CT and MRI, their findings should be provided. After receiving all the data, the specialist prescribes a study or selects another option if necessary.
On the day of the examination, you should refrain from eating food for at least 3 hours. You are allowed to drink plain water. If the patient has been prescribed beta-blocker drugs, he should inform the doctor about them. They may be required during the examination.
The price for coronary angiography of the heart in Moscow starts from 10 thousand rubles. It is worth keeping in mind that some clinics indicate the cost without taking into account contrast.
CT chest
MSCT is the most accurate and fastest method for diagnosing diseases of the chest organs (trachea, bronchi, lungs, mediastinum) - lung cancer, pneumonia, tuberculosis, emphysema, bronchiectasis, pleurisy, interstitial lung diseases.
- Clarifying study after chest x-ray.
- Screening and diagnosis of any diseases of the lungs and mediastinum.
- Diagnosis of the presence and prevalence of tumors of the chest organs, as well as assessment of the effectiveness of antitumor treatment.
- Radiotherapy planning.
- Assessment of the condition of blood vessels, lungs, ribs and spine after injury.
- Diagnosis of pulmonary embolism (using CT angiopulmonography with intravenous contrast).
Contraindications
To avoid complications, the doctor carefully collects anamnesis. There are a number of reasons why the examination cannot be carried out. These include:
- Intolerance to iodine-containing drugs.
- Pathologies of the thyroid gland.
- Pregnancy at any stage.
- Abnormalities in the regularity or frequency of the heart rhythm.
- Rapid heart rate of more than 90 beats per minute.
- Kidney failure.
- Diabetes mellitus with glucose levels more than 14 mmol/l.
There are also less serious contraindications that the doctor should pay attention to. These are:
- taking medications based on metformin and dipyridamole;
- taking medications with a toxic effect on the kidneys (many painkillers, aminoglycosides);
- the patient's inability to hold his breath;
- psychical deviations;
- excess weight exceeding the norm for a CT scanner.
What allows you to research what diseases to identify
Using MSCT of the heart, you can accurately diagnose:
- Ischemic disease;
- Aneurysms;
- Pathologies of the cardiac aorta and coronary arteries of the heart;
- Congenital anomalies of the cardiovascular system;
- Acquired heart defects (for example, calcification of the aortic valve);
- Diseases of peripheral cardiac arteries;
- Pulmonary thromboembolism.
The examination is often carried out in acute conditions of the patient, which are accompanied by severe pain in the thoracic region - pneumothorax, myocardial ischemia, etc.
How is the examination carried out?
Before performing a coronary angiography in a hospital, you should remove from your body all objects or clothing with metal in the chest area (especially bras). After this, a catheter is inserted into the cubital vein, through which a contrast agent is supplied during the procedure. The patient lies in a comfortable position on his back and puts his hands behind his head, after which a tube from the tomograph is attached to the catheter to dose contrast during the examination. The person is only required to hold his breath on command and not be nervous.
During contrast administration, a metallic taste may be felt in the mouth and moderate warmth in the chest area, spreading throughout the body. There should be no pain. Otherwise, you should immediately contact the doctor performing the manipulations.
Indications:
- identified foci of calcification (calcification) of the valvular apparatus of the heart, cardiac muscle (myocardium) or serous membrane of the heart (pericardium) when performing computed tomography of the chest;
- old post-infarction scars, aneurysms of the great vessels or suspected presence of blood clots in the cavities of the heart;
- high calcium index values when assessing coronary calcification (CT “calcium scoring”);
- suspicion of abnormal development of heart vessels or heart valve insufficiency, for example when performing echocardiography;
- chest pain of unknown etiology, atypical pain;
- the appearance of primary or repeated symptoms of angina pectoris;
- deviation from normal indicators of electrocardiography, stress tests, laboratory tests;
- the need to assess the blood supply to the heart muscle (myocardium) after surgical interventions (coronary artery bypass grafting, coronary artery stenting).
[/td]
The high prevalence of cardiovascular diseases and the first place among the causes of mortality in developed countries makes preventive measures and early diagnosis of heart disease . MSCT of the coronary arteries can be performed as a screening during a preventive (dispensary) examination of a person. Atherosclerosis of the coronary arteries is the main cause of the development of coronary heart disease (coronary heart disease) and myocardial infarction. Modern medicine has a wide range of diagnostic capabilities. And with the advent of high-speed multislice computed tomography (MSCT), a completely new, unique opportunity has emerged for non-invasive assessment of the condition of the coronary arteries, which does not require hospitalization of the patient to a hospital for a complex and unsafe surgical procedure (angiography).
MSCT examination takes only a few minutes, does not require additional preparation, and does not cause pain or emotional anxiety. In addition to assessing the condition of the heart vessels ( coronary “tree” ), MSCT of the coronary arteries provides the doctor with additional equally important information, which allows him to assess the condition of the heart as a whole, and develop tactics for further examination and treatment. MSCT allows you to evaluate the morphological structure of an atherosclerotic plaque , study the valve structures of the heart (calcification of the leaflets, anomalies of valve development), identify myocardial lesions (hypertrophy, scars), and assess the condition of the cavities of the heart and pericardium. Valuable information is provided by determining the function of the left ventricular myocardium with identifying areas of impaired contractility.
Price
You can see prices for services
The cost of contrast is added to the cost of the study.
Preparation for CT coronary angiography
| Pulse | Does not depend on mass:
| |
| Diet on the day of the study |
| |
| Take with you |
| |
| Keep in mind | if the pulse is high, the study may not take place | |
Indications:
[td]
- high blood cholesterol levels;
- burdened heredity;
- the patient has diabetes;
- high blood pressure (hypertension);
- long-term smoking;
- overweight or obesity;
- insufficient physical activity.
Multislice computed tomography (MSCT) of the coronary arteries (“CT coronary angiography”, “CT cardiac angiography”)
MSCT coronary angiography with contrast enhancement, construction of volumetric (3D) reconstructions and determination of coronary calcification is a non-invasive method for visualizing the arteries of the heart. At the same time, the degree of patency of the artery of the heart (coronary arteries) and their anatomical features are determined with high accuracy, and the overall level of blood supply to the heart muscle (myocardium) is also assessed. Multislice computed tomography (MSCT) of the coronary arteries can serve as an alternative to X-ray angio-coronary angiography.
Possibilities of MSCT in diagnostics.
MSCT is used in the diagnosis of the cardiovascular system in [2,7,9,15]:
- Coronary heart disease (CHD)
- Diseases of the aorta (coarctation, aneurysm, dissection, etc.)
- Damage to peripheral arteries (obliterating atherosclerosis of the arteries of the lower extremities, atherosclerosis of the carotid arteries, etc.)
- Pulmonary embolism
- Congenital anomalies of the cardiovascular system
- Acquired heart defects, for example, calcification of the aortic valve with the development of stenosis or insufficiency, etc., including for planning further surgical treatment ( TAVI ) [75]
I. Coronary arteries of the heart
The high-resolution ability of MSCT allows:
A) reliably visualize the coronary arteries [2,3, 4,18], with clarification of the localization of atherosclerotic lesions, identifying abnormalities in the development of the coronary vessels of the heart (Fig. No. 1).
B) determine the viability of coronary artery bypass grafts and intravascular endoprostheses (stents) [7,8,17,29,33] (Fig. No. 4).
C) calculate the CI [1,2,3,12] in order to clarify the prognosis of the disease.
D) to note disturbances in perfusion and myocardial viability in patients in the early and later stages of myocardial infarction [2,13,24,45,50].
D) assess the contractility of the heart [2,11,13,21,25].
E) study the condition of the pericardium, heart valves [2,10]
Rice. No. 1 . 3-D reconstruction of the coronary arteries using MSCT. The trunk of the left coronary artery, permanent abdomen, and rectal artery is visualized.
Visualization of atherosclerotic lesions of the coronary arteries using MSCT is an alternative to invasive coronary angiography (CAG) (Fig. 5, 6) and is used both in proven IHD [2,3,12,40], and in cases of suspected IHD, and in asymptomatic patients [2,14,67], for the purpose of diagnosis, identification of risk groups and determination of their further prognosis.
Including indications for the study are [2,3,40,42]:
1. atypical chest pain, including those with risk factors:
- arterial hypertension,
- hyperlipidemia,
- obesity,
- diabetes,
- smoking,
- high CI,
- family history of coronary heart disease, sudden death, peripheral artery disease.
2. acute coronary syndromes, myocardial infarction without ST elevation to assess damage to the coronary arteries of the heart [16]. MSCT allows you to diagnose possible complications during myocardial infarction, for example, the development of a left ventricular aneurysm (Fig. No. 2).
Rice. No. 2. MSCT of the heart. Aneurysm at the apex of the left ventricle (arrow)
3. conditions after coronary artery bypass grafting (CABG) or percutaneous transluminal angioplasty of the coronary arteries (PTCA) with stent implantation to determine the viability of coronary artery bypass grafts or intravascular endoprostheses [7,8] (Fig. No. 3, 4).
Rice. No. 3. 3-D reconstruction of a patient after CABG. Arrows indicate aorto-coronary bypass grafts and mammary-coronary bypass graft.

Rice. No. 4. On the right is a 3-D reconstruction of a patient after angioplasty with stent implantation in the RCA. Stent without signs of restenosis.

Rice. No. 5, 6. MSCT (photo on the left) and CAG (photo on the right) of the coronary arteries. Hemodynamically significant stenosis of the LAD (arrows).
II. Extra- and intracranial vessels
MSCT of extra- and intracranial vessels is performed for vascular lesions of the brain, cerebrovascular accidents - these are indications for studying the anatomy of intracranial vessels, neck vessels in order to exclude developmental anomalies, including identifying all kinds of arterial malformations (Fig. 7-10), as well as to exclude atherosclerotic lesions of extra- and intracranial arteries in patients who have suffered acute cerebrovascular accident or transient ischemic attacks (Fig. 11, 12) [2,3]. Simultaneously with the examination of the arteries, a reconstruction of the anatomy of the brain is carried out, identifying the smallest damage (tumors, hematomas, etc.), ranging in size from 0.4-0.6 mm. Accurate diagnosis using MSCT will allow us to determine the cause of the disease and the location of the lesion, which is necessary to determine the tactics of further treatment.

Rice. No. 7-10. Diagnosed aneurysm of the middle cerebral artery on MSCT of the intracranial arteries (arrows).

Rice. No. 11, 12. MSCT 3-D reconstruction of the carotid arteries. Stenosis of the left internal carotid artery (arrow).
Together with ultrasound data, CT of the brachiocephalic arteries allows us to assess the condition and composition of the atherosclerotic plaque.
III. Aortic arch, thoracic and abdominal aorta
Detection or suspicion of anomalies in the development of the aorta and its branches, the consequences of syphilitic aortitis, atherosclerotic lesions of the aorta with the development of an aneurysm - this is the entire list of diseases that require 64 MSCT. The possibility of visualizing the dissection of an aortic aneurysm of any location has also been shown[2,3,52]. Computed tomography of the aorta is also of great importance for assessing the effectiveness of treatment of aneurysms, including after endoprosthetics of thoracoabdominal aortic aneurysms with stent grafts. (Fig. No. 15-18)

Rice. No. 13, 14. MSCT of the thoracic aorta. Aneurysm of the descending aorta
Rice. No. 15-18. MSCT of the abdominal aorta and its branches. Aneurysm of the infrarenal aorta and subsequent MSCT monitoring of effectiveness after surgical endovascular treatment. White arrows indicate aortic aneurysm. Yellow arrows indicate the stent graft, with no signs of leakage.
An interesting clinical case described by Leschka S. et al. (2005) [66] – during endovascular correction for coarctation of the aorta, the patient developed pain in the back, an urgently performed 64 MSCT made it possible to diagnose acute aortic dissection, after which the patient underwent open aortoplasty.
The possibility of highly accurate anatomical and topical diagnostics, the reliability, and speed of the information obtained determine the need to refer patients with such pathology to MSCT. Also, CT of the aorta is used for monitoring after surgical treatment of its coarctation (Fig. No. 19)[55].

Rice. No. 19. MSCT of the thoracic aorta, monitoring the effectiveness after surgical treatment of aortic coarctation. The arrow indicates a linear aortic prosthesis.
The next indication for examination of the abdominal aorta and its branches is malignant arterial hypertension to identify renal artery stenosis [2,3] (Figure No. 20). Also, CT examination allows one to evaluate the effectiveness of surgical treatment of these lesions of the renal arteries (Fig. No. 21).
The clinical picture of stenotic lesions of the aortic branches also requires clarification; such patients may undergo invasive aortoangiography (AAG) or the more convenient MSCT.

Rice. No. 20, 21. MSCT in a patient with renovascular hypertension. Stenosis of the right renal artery (narrow arrow). The wide arrow points to the stent, with no evidence of restenosis.
IV. Peripheral arteries of the upper and lower extremities
The clinical picture of peripheral artery disease, especially in diabetes mellitus complicated by diabetic angiopathy, is an indication for referral to MSCT. The next group of patients are experienced smokers. Direct damage to the endothelium of the vascular wall has been proven when smoking tobacco, so the incidence of occlusive arterial diseases in such patients is much higher. The results of the study will help the doctor in choosing therapy, including minimally invasive endosurgical treatment.

Rice. No. 22-25. 3-D reconstruction of peripheral arteries using MSCT. Multiple atherosclerotic lesions.
Rice. No. 26, 27. MSCT of peripheral arteries. Evaluation of treatment effectiveness. Stent with signs of restenosis.
V. MSCT of the heart
In addition to direct visualization of the coronary arteries, simultaneously, in one study, MSCT allows non-invasive diagnosis of various anomalies of the heart and nearby vessels, including valvular pathology [10,15,26]. In this situation, the method is used for more accurate anatomical diagnosis necessary for further treatment, and also allows one study to replace many others. For example, in a patient with degenerative aortic valve stenosis, an aneurysm of the initial aorta, before the planned replacement of the valve and the initial aorta, it is necessary to evaluate the coronary reserve for possible further simultaneous implementation of prosthetics with CABG. MSCT will replace diagnostic CAG, AAG and echocardiography, which will significantly speed up the time of examining a patient without reducing the diagnostic value.

Rice. No. 28. Anomaly of the development of the coronary arteries. The LCA originates from the RCA.
The speed and reliability of the study are important in many clinical situations; for example, the possibility of diagnosing a ruptured aneurysm of the sinus of Valsalva in acute myocardial infarction using MSCT is described (Fig. No. 29). Interestingly, in the presented case, the rupture was not detected during echocardiography [51]. Fast and accurate diagnosis using MSCT will guide the doctor in choosing the appropriate treatment tactics without wasting precious time.

Rice. No. 29. CT scan of the heart and coronary arteries. Dissection of the ascending aorta.
Using MSCT, the possibility of visualizing the bicuspid aortic valve and identifying vegetations on the aortic valve in infective endocarditis has been described [43]. But these conditions are more often a finding on CT (Fig. No. 30) and it is advisable to diagnose them using transesophageal echocardiography.
It is known that patients with a bicuspid aortic valve have a high risk of developing an aneurysm of the ascending aorta and its dissection, therefore, in such patients, accurate diagnosis of the lesion is important for timely surgical correction of this pathology.
Rice. No. 30. Infectious endocarditis. Vegetations on the aortic valve (arrow)
Taking into account the high visual ability of the method, MSCT can be widely used in patients with various heart rhythm disorders [2,27,54]. Especially when:
- Studying the condition of the heart cavities in patients with paroxysmal atrial fibrillation or other rhythm disturbances.
- Studies before and after radiofrequency ablation to assess possible changes in the pulmonary veins and cardiac anatomy [65] (Fig. No. 31, 32)
Identification of a thrombus in the left atrial appendage (Fig. No. 33). In patients with paroxysmal forms of atrial fibrillation, in order to decide on further treatment tactics, it is necessary to clarify the presence of a thrombus in the left atrial appendage. The usual diagnostic method is transesophageal echocardiography. An alternative to transesophageal echocardiography is MSCT.

Rice. No. 31, 32. CT of the pulmonary veins.

Rice. No. 33. CT scan of the heart, thrombus in the left atrial appendage (arrow).
Another direction for MSCT is the diagnosis of cardiac tumors, myocardial infiltration in amyloidosis, sarcoidosis [31,53] (Fig. No. 34, 35, 36). MSCT in a matter of minutes will make it possible to clarify the localization of heart damage with a high degree of reliability, and will also provide an additional opportunity to study the state of blood circulation in the coronary arteries of the heart, and evaluate pericardial structures and valves.
Rice. No. 34. MSCT of the heart, left atrial myxoma (arrow).

Rice. No. 35, 36. MSCT of the heart, tumor of the right atrium (arrow). According to histological examination - angiosarcoma.
Exudative or restrictive pericarditis or suspected pericardial diseases, including inflammatory lesions of the myocardium, are also in the area of application of MSCT [2] (Fig. No. 37).
Rice. No. 37. CT scan of the heart. Fluid in the pericardium, 15 mm thick.
VI . Pulmonary vessels
MSCT allows you to visualize other body systems in addition to the heart, therefore additional visualization of the pulmonary artery and lungs (Fig. No. 38, 39) allows you to diagnose pulmonary embolism ( PE) (Fig. No. 40, 41) [19,52]. The high reliability and sensitivity of the MSCT method, the fast speed of the study, will allow the doctor to correctly diagnose such a formidable disease and begin the necessary therapy on time.

Rice. No. 38, 39. MSCT visualization of the heart, lungs, pulmonary veins and arteries.

Rice. No. 40, 41. MSCT of the pulmonary artery. Massive bilateral pulmonary embolism. Arrows indicate blood clots.
Research methodology.
MSCT angiography is based on the technique of scanning during the arterial phase during the rapid passage of the contrast agent.
To prepare the patient for the study, the following is required: hydration before the study (start drinking water several hours before the procedure), discontinuation of certain nephrotoxic drugs, and a mandatory blood test for creatinine to assess kidney function. MSCT is performed on an outpatient basis. The patient is in a supine position (Fig. No. 42). After a preliminary scan, which is necessary to accurately determine the location of the organs of interest in the area being examined, a contrast agent containing iodine is injected intravenously as a bolus, then scanning begins with a slight delay, within a few seconds, and then the received data is processed by a computer. The total patient examination time takes about 10-20 minutes. The final data is subsequently available for analysis and imaging. And then the doctor analyzes the results on a special workstation.
The development of the method was facilitated by:
- high diagnostic value,
- relative ease of implementation,
- speed of information acquisition
- convenience for the patient (no need for premedication, preliminary tests, etc.).
- and also that MSCT is the first non-invasive technique for visualizing the coronary arteries that does not require hospitalization, without the risk of intra- and postoperative complications.
Rice. No. 42. Research methodology
Comparison with other imaging methods.
Currently in medical practice for visualization of the heart and vascular bed are used:
- ultrasound (ECHO-Doppler, intravascular study),
- magnetic resonance imaging (MRI),
- invasive AAG and CAG,
- myocardial scintigraphy
- CT scan.
As is known, invasive AAG and CAG are the “gold standard” in the diagnosis of arterial lesions, therefore, with the advent of MSCT of the coronary arteries, researchers were tasked with comparing the results obtained with data from invasive imaging methods [2,5,20,47,48].
A large number of studies devoted to this issue have shown that 64 multislice CT of the coronary arteries in the diagnosis of hemodynamically significant stenotic lesions (stenosis >=50%) has, in comparison with CAG: sensitivity 94%-100%, specificity 95%-97%, positive predictive value 87%-97%, negative predictive value 99%-100% [3,20,23,30,35,47,48]. The presented results confirmed the identity of the obtained results of MSCT and CAG in the diagnosis of atherosclerosis of the coronary arteries (Fig. No. 5, 42).
The next “gold” standard, but in the diagnosis of global and regional left ventricular function, is MRI. Studies conducted on direct comparison of high-resolution MRI with 64-MSCT showed statistical consistency of the data obtained on the study of the state of the heart in patients with myocardial infarction [13]. In this work, Baks T et al. showed that 64 MSCT reliably determines the area of the zone of myocardial necrosis in comparison with 1.5 T MRI.
The most common method for diagnosing CAD is to perform exercise testing. A direct comparison of Dewey M. et al. (2006) of the exercise tolerance test in 80 patients with 16 MSCT showed a significant advantage of the latter technique in detecting coronary heart disease: sensitivity was 73% versus 91%, specificity 31% versus 83% (p = 0.039) (CAG completed the study in order to accurately verify IHD) [67]. Summarizing the above, we note that even 16 MSCT has a higher diagnostic value than stress tests for recording lesions of the coronary arteries.
A direct comparison of 16-spiral CT of the coronary arteries with CAG showed that the sensitivity, specificity, positive and negative predictive values were 85-89%, 98%, 90-91%, 96-98%, respectively [36,37,38, 41], with a higher percentage of motion artifacts proven than in 64 MSCT [22]. These data indicated a lower diagnostic ability of 16-spiral CT than that of 64-MSCT [6,22,32]. Garcia MJ et al (2006) after studying 187 patients with high coronary CI (more than 600), noted that the sensitivity of 16-helix CT was in the range from 89% to 94%, and the specificity ranged from 51% to 67%. In conclusion, the authors point out that 16-spiral CT is not an alternative to diagnostic coronary angiography, due to the large number of undiagnosed cases of lesions [60].
A comparison of two techniques: ventriculography and 64 MSCT used to study global left ventricular function showed statistical identity of the data obtained [21].
A comparison of 64 MSCT and intravascular ultrasound for stenosis of the internal carotid artery showed significant superiority of MSCT in verifying the nature of the atherosclerotic plaque [58].
Thus, modern MSCT is not inferior to invasive methods, which are the “gold standard” in the diagnosis of diseases of the peripheral and coronary arteries, CAG and AAG. MSCT has a number of advantages over selective coronary angiography:
- in the relative simplicity of performing the diagnostic procedure,
- absence of possible intra- and post-operative complications,
- speed of research and obtaining information,
- no need for hospitalization and
- carrying out premedication, which ultimately determines the convenience for the patient.
- lower risk of contra-induced nephropathy.
In addition to the above advantages over coronary angiography, MSCT provides additional characteristics of the atherosclerotic plaque (detection of “soft” plaques, degree of calcification, etc.) [2], determines the systolic function of the heart (based on the diastolic and systolic volumes of the left and right ventricle, an accurate ejection fraction calculation) (Fig. No. 42, reveals areas of dyskinesia of the left ventricular myocardium (when constructing a 4-dimensional volumetric image), with an additional assessment of the anatomy of the heart and blood vessels. And, which is important for prognosis, MSCT retains the ability to determine perfusion capacity and evaluate myocardial viability [2,13,24,45,50].This is especially important for patients with myocardial infarction and patients with heart failure.

Rice. No. 42. Assessment of ejection fraction with CT of the coronary arteries.
A comparison by Khare KR (2006) of two techniques, stress echocardiography with 64 MSCT, showed higher efficiency of the latter in diagnosing the causes of chest pain [49].
Gerber TC et al. (2005) noted the identity of diagnostic data when using transthoracic echocardiography and 16 MSCT in recording prolapse of the posterior mitral valve leaflet [61] (Fig. No. 43). Alkadhi H. et al. (2006) [62] and Gudrun M. et al. (2006) [63] to study aortic valve stenosis. The authors note 100% sensitivity and 97.3% specificity of MSCT in the diagnosis of heart valve diseases.
Messika-Zeitoun D. et al. (2006), when comparing the capabilities of transthoracic echocardiography and 16 MSCT in studying the area of the mitral valve in mitral stenosis, indicated a more accurate measurement and anatomical and visual superiority of MSCT over echocardiography, and suggested using this study in patients with poor ultrasound window or before replacement of affected valves [64].
Similar data were presented by Gilard M. et al (206) [59], who suggested that all patients undergo MSCT before aortic valve replacement, which allows one to simultaneously study the coronary reserve of the heart and the anatomical characteristics of the aortic valve.
Monique RM et al. (2005) published the results of a direct comparison of transthoracic echocardiography and MSCT in 42 patients before ablation of the pulmonary veins: the measured diameter of the pulmonary veins was comparable, but MSCT showed a higher frequency of identifying additional branches of the pulmonary arteries [65].
Thus, MSCT is not inferior to ultrasound examination of the heart in studying lesions of the valves and heart structures, while having significant superiority in image quality plus the possibility of simultaneous examination of the coronary arteries, with a characterological assessment of the atherosclerotic plaque and the ability to identify myocardial perfusion disorders.
The capabilities of 16 MSCT in the diagnosis of intracranial aneurysms were shown by Wintermark M. et al. When compared with AAG, it turned out that the sensitivity, specificity, and accuracy of the results of 16 MSCT were 94.8%, 95.2% and 94.9%, respectively [74].
Fraioli F. et al. (2006) when examining 50 patients with renal artery stenosis confirmed by AAH, noted high sensitivity, specificity, accuracy, positive and negative predictive value of MSCT (100%, 98.6%, 96.9%, 98.2% and 97.8%, respectively) [73]. The authors of the study recommend wider use of MSCT for diagnosing this pathology.
A number of researchers compared the effectiveness of 16 MSCT with invasive AAG in the examination of stenotic atherosclerosis of the vessels of the lower extremities [69,70,71,72]. Bui TD et al. (2006) noted that for all segments the sensitivity and specificity were: for stenosis <50% - 86 and 90%, for 50-99% - 79% and 89%, for occlusions - 85% and 98%, respectively [69] . Xiao-dan Zhang et al (2006), when assessing segments with >50% stenosis, indicated that the sensitivity was 94.3%, specificity 98.4%, positive predictive value 92.7%, negative predictive value 98.7%[70]. Thus, scientists have proven the comparability of the results of 16 MSCT with AAG in the diagnosis of lesions of peripheral arteries [69,70,71,72], noting significantly less time spent for the study: 2.5 +/- 0.3 minutes with 16 MSCT versus 37.5 +/- 5.2 in AAG, p = 0.006[71].
The results of a comparison of the diagnostic capabilities of 64-MSCT and other research methods are presented in Table No. 1 [2]:
Table No. 1. Comparison of the diagnostic capabilities of 64-MSCT and other research methods.
| ECHO-DopplerCG | KAG | MSCT | MRI | |
| Anatomy of the coronary arteries | — | +++ | +++ | RM |
| Systolic heart function | ++ | — | ++ | +++ |
| Identification of areas of myocardial dyskinesia | ++ | ventriculography | ++ | +++ |
| Anatomy of the heart and blood vessels | ++ | — | +++ | +++ |
| Characteristics of plaque | Intravascular study only | — | ++ | RM |
| Myocardial perfusion | — | — | + | +++ |
| Myocardial viability | ++ | — | RM | +++ |
RM – further development of the method
As can be seen from the table presented, MSCT includes all the capabilities of other imaging methods, being currently the most universal diagnostic method, while maintaining high safety, information content and convenience for the patient.
Restrictions on the use of MSCT
At the same time, MSCT also has some limitations in use, similar to CAG and AAG. The following contraindications exist [3,17]:
Absolute:
1. severe and moderate allergic reaction to iodine-containing contrast agents.
Relative:
2. renal failure (significant decrease in plasma creatinine clearance). 3. pregnancy 4. severe clinical condition of the patient, including severe CHF. 5. the patient’s inability to assume a supine position. 6. the patient’s inability to hold his breath for up to 15 seconds. 7. severe obesity, body weight more than 130 kg. 8. multiple myeloma. 9. uncompensated hyperthyroidism 10. permanent form of atrial fibrillation and frequent extrasystole when diagnosing coronary arteries.