Shilov G.N., Krotov A.V., Dokukina T.V. State Institution "Republican Scientific and Practical Center for Mental Health"
In the literature (Pandey A. et all, 2004), the issue of using one or another neuroimaging method (primarily CT and MRI, as the most common and accessible methods) to identify diseases with developmental disorders of the central nervous system (CDNSD) is quite widely discussed. which, in particular, include autism spectrum disorders (ASD), usually supervised by psychiatric practice.
It is well known from literary sources (Shalock RL et all 2007, Gillberg C., 2000; Bashina V.M., 1999) that autism is a disease with significant deviations in reciprocal relationships (i.e. in the development of communication), as well as limited behavior, interests, imagination and early onset of the disease, usually before 3-5 years (Morozov S.A., 2002; Lebedinskaya K.S., Nikolskaya O.S., 1991; Shchipitsyna L.M., 2001) . Currently (according to ICD-10), autism in its clinical manifestations is classified into: childhood autism; atypical autism; Rett syndrome; other childhood disintegrative disorder; hyperactive disorder combined with mental retardation and stereotypic movements; Asperger's syndrome (see diagram 1).
It is believed that a child with CRNS has impaired brain function, which is probably based on developmental disorders in the form of pathological morphogenesis or histogenesis. It is believed that using MRI it is possible to identify minor and major malformations of the brain, which indicate the participation of the identified structural changes in the pathogenesis of NRNNS (Decobert F. et all, 2005). However, it is possible to make an etiological and/or syndromic diagnosis based only on MRI data only in a small group of patients (0-3.9%). ZRCNSL is determined by many different etiological factors, which significantly complicates the diagnosis. At the same time, the value of the results of neuroimaging studies, such as magnetic resonance imaging (MRI), in the analysis of patients with SRCNS remains uncertain, given that the pathological changes that are usually detected in children with SRCNS are not specific enough.
However, the range of recommendations for MRI varies from examining all patients with CRNS (Shaefer GB, 1998) to examining only patients with indications for clinical examination using MRI (van Karnebeek CD et all, 2005). It is believed that the most important indications for neuroimaging are pathological changes in head size, the presence of signs of various types of central nervous system anomalies, certain neurological and mental symptoms and syndromes that are identified during the collection of anamnestic data and/or physical examination, indicating a high probability of structural pathology of the brain brain
As for ASD itself, it is now generally accepted that in most cases the occurrence of this pathology is the result of a combination of genetic predisposition and exogenous trigger factors caused by a number of reasons, such as viruses, toxins, immune-allergic stress, etc. (Van Gent et all, 1997; Comi AM et al., 1999; Warren, R.P., et al., 1996; M. Kontstantareas et al., 1987; Gassen A.N., 1999; Singh V.K. et al. ., 1997).
MRI of a child's brain
The purpose of the study was to outline the role and significance of MRI (as the most harmless and informative method for studying the central nervous system in children) in the diagnosis of spinal cord nervous system syndrome, as well as to identify the most important trigger exogenous factors in the occurrence of ASD.
Materials and methods
The studies were carried out on an “Obraz 2 M” tomograph (RF, 1998) with a magnetic field strength of 0.14 T in the sequence T1W, T2W axial and sagittal planes (according to indications - with the use of intravenous anesthesia or sedation).
A total of 61 children with ASD aged 3 to 15 years were examined. The diagnosis of children with ASD was established in accordance with the ICD-10 criteria and on the basis of a detailed clinical examination: the psychological, psychiatric and neurological status was studied, a mandatory examination by a pediatrician and consultations with other specialists, magnetic resonance imaging (MRI) and an electroencephalogram (EEG) were carried out. The clinical picture of ASD was dominated by: qualitative impairment of social interaction, repetitive limited stereotypic behavior, impairments in the cognitive sphere, regardless of the presence or absence of mental retardation; the onset of the disease was usually noted in the first 3 years of life. The spectrum of diagnostic pathology included: childhood autism - 28 people; atypical autism – 25 people; Rett syndrome - 1 person; Heller's syndrome - 2 people; Asperger's syndrome-5 people.
Results and discussion
The results of MRI scans of the brain were assessed according to the detected structural disorders, taking into account their relationship with characteristic clinical symptoms and signs (see Diagram 2 - the most quantitatively significant groups from the entire spectrum of ASD are presented).
In the group of those examined with a diagnosis of childhood autism, which included 28 patients (which accounted for 46% of the total number of patients with ASD), MRI signs of structural abnormalities were found, which were regarded as: 1. consequences of a previous neuroinfection (including asymmetry of the lateral ventricles) – in 9 (32.1%) cases 2. inflammatory changes in the paranasal sinuses and structures of the temporal bones – in 5 (17.9%) cases 3. changes corresponding to a combination of signs of the consequences of a previous neuroinfection and signs of inflammation in the paranasal sinuses and structures of the temporal bones bones were determined in 4 (14.3%) cases 4. midline cysts - in 3 (10.7%) cases 5. changes corresponding to the set of signs of the consequences of a neuroinfection with midline cysts in 1 (3.6%) case 6. changes , corresponding to a set of signs of inflammation in the paranasal sinuses and structures of the temporal bones with midline cysts in 1 (3.6%) case. In this case, a normal MRI picture was determined in 5 (17.9%) cases.
How to prepare for an MRI under general anesthesia?
- Preliminarily undergo diagnostics: general blood test, general urinalysis, blood sugar test, ECG, get a consultation with an anesthesiologist.
- The day before, adjust your diet, including only light dishes in the menu. On the day of the study:
- Adults - do not eat food 6-8 hours before;
- Children over one year old – 6 hours;
- Liquid (preferably clean water) – 3-4 hours
- To undergo the examination, you should follow the standard rules for preparing for MRI:
- It is not advisable to apply makeup or wear jewelry before the procedure. If you wear dentures, they must be removed during the examination. Contact lenses should also be removed (MRI under anesthesia);
- Clothing should be comfortable, without metal elements (buttons, locks, jewelry, bra);
- Remove all metal objects (earrings, chains, rings, brooches, hairpins, hairpins, piercings, pens). If it is impossible to remove the wedding rings, the gold can be left, because... it does not distort images;
- Remove watches, mobile phone, credit cards, money;
- Remove the hearing aid.
After research:
You can drink water only after 30 minutes, eat food after 2 hours.
Important!
For 24 hours, do not drive a vehicle or perform hazardous activities that require increased concentration and high speed of psychomotor reactions.
Magnetic resonance imaging for autism
In the group of patients diagnosed with atypical autism, which included 25 children, which accounted for 41% of the total number of patients with ASD, MRI signs of structural abnormalities were found, which were regarded as: 1. consequences of a previous neuroinfection (including asymmetry of the lateral ventricles) – in 9 (36%) cases 2. inflammatory changes in the paranasal sinuses and in the structures of the temporal bones – in 5 (20%) cases 3. changes corresponding to a combination of signs of the consequences of a previous neuroinfection and signs of inflammation in the paranasal sinuses and in the structures of the temporal bones bones, were determined in 4 (16%) cases 4. changes corresponding to a set of signs of the consequences of a neuroinfection with midline cysts in 2 (8%) cases. In this case, a normal MRI picture was determined in 5 (20%) cases.
Rett syndrome was diagnosed in 1 child (MRI was normal).
The group diagnosed with childhood disintegrative disorder was also small - 2 cases, which accounted for 3% of the total number of patients with ASD: in 1 case, signs of the consequences of a neuroinfection were revealed (including asymmetry of the lateral ventricles), in 1 case - changes corresponding a set of signs of the consequences of a previous neuroinfection and signs of inflammation in the paranasal sinuses and structures of the temporal bones.
In the group of patients diagnosed with Asperger's syndrome, which included 5 patients (which is 8% of the total number of patients with ASD), the following MRI signs of structural abnormalities were found: 1. consequences of a previous neuroinfection (including asymmetry of the lateral ventricles) - in 2 (40%) cases 2. changes corresponding to a combination of signs of the consequences of a previous neuroinfection and signs of inflammation in the paranasal sinuses and in the structures of the temporal bones were determined in 1 (20%) case 3. midline cysts in 1 (20%) case. In this case, a normal MRI picture was determined in 1 (20%) case.
Of the study group of 61 people, 21 (34.4%) patients showed signs of the consequences of a neuroinfection; 24 (39.3%) had signs of inflammation in the paranasal sinuses and structures of the temporal bones; in 8 (13.1%) the presence of midline cysts was determined; in 12 (19.7%) there was an MRI picture without signs of pathology in the brain and paranasal sinuses, as well as the structures of the temporal bones.
Thus, in 45 patients (which amounted to 73.7% of the total) with an established diagnosis of childhood autism and atypical autism, MRI signs of the consequences of a previous neuroinfection and MRI signs of inflammatory changes in the paranasal sinuses and/or cells of the mastoid processes of the temporal bone were revealed (see .diagram 2.).
Information for patients during research
The RCT office is open 24 hours a day. At night, studies are carried out mainly for emergency indications (traumatic injuries to the skull and brain, abdominal cavity, cerebral hemorrhages, etc.), planned studies are carried out less often
The X-ray computed tomography room of the Children's Clinical Hospital of the Ministry of Health of the Republic of Tatarstan is the leader in the republic in computed tomography of children. For children under 5 years of age and restless patients in serious condition, RCT examinations are performed under sedation or anesthesia.
In the RCT room, studies are also carried out on adult patients in Kazan and the republic.
In the X-ray computed tomography room, examinations of various organs and systems are carried out (brain and spinal cord, skull bones, paranasal sinuses, temporal bones, spine, soft tissues and organs of the neck, lungs and bronchi, mediastinal organs, abdominal organs and retroperitoneal space, organs pelvis, bones and soft tissues of the trunk and limbs, organs of vision, joints). CT angiographic studies are carried out to identify vascular anomalies, to clarify the nature of the blood supply to identified tumors and their relationship with the great vessels, CT angiographic studies for portal hypertension, CT angiographic studies of pulmonary vessels for the diagnosis of pulmonary embolism, CT studies of the heart for congenital defects and CT studies of the heart with coronary angiography .
Computed tomography is prescribed by a doctor, taking into account clinical data and all previous research methods (in most cases, preliminary radiography or ultrasound is necessary). This approach allows you to more accurately determine the area of interest, make research targeted, avoid conducting studies without indications, and reduce the dose of radiation exposure.
Indications for MSCT
Examination of the chest organs
—infectious lung diseases (pneumonia, infectious destruction, respiratory tuberculosis, pneumoconiosis, parasitic infections);
- lung tumors;
-metastatic lesions of the lungs;
-bronchial diseases (bronchiectasis, cysts, cicatricial bronchial stenosis, bronchial foreign bodies, bronchiolitis);
- pulmonary circulation disorders (pulmonary embolism, pulmonary infarction, septic pulmonary embolism, pulmonary vascular anomalies);
- interstitial lung diseases (alveolitis, lymphogenous carcinomatosis, histiocytosis, sarcoidosis, silicosis and anthracosis, hypersensitivity pneumonitis, emphysema);
- diseases and damage to the thoracic aorta and its branches;
— extrapulmonary aptological processes: diseases of the mediastinum, pathology of the pleura (pleural effusion, pneumothorax, pleural tumors), chest wall
Examination of the abdominal organs and retroperitoneal space
- primary or secondary tumor damage to the liver and biliary ducts, fatty liver, abscesses, cysts, including parasitic ones, cirrhosis of the liver;
- diseases of the biliary tract;
-hepatomegaly of unknown etiology;
- damage to the abdominal organs and retroperitoneal space;
- diseases of the pancreas;
- diseases of the spleen, splenomegaly of unknown etiology;
- diseases and damage to the kidneys and urinary tract;
Anomalies of the abdominal cavity and retroperitoneal space;
- diseases of the adrenal glands;
- diseases and damage to the abdominal aorta and its branches;
- diseases and damage to the inferior vena cava, portal veins and their tributaries (for example, portal hypertension, thrombosis).
Attention! Before examining the abdominal organs, retroperitoneum and pelvis, special preparation is required.
Examination of the pelvic organs
- diseases and injuries of the urinary tract;
- diseases of the uterus and appendages (in particular, tumor and inflammatory diseases, establishing zones of their prevalence);
- diseases of the prostate gland (mainly for diagnosing the prevalence of the tumor process);
-structure, condition of regional lymph nodes;
- diseases and damage to the iliac vessels (aneurysm, stenosis, dissecting aneurysm);
- diseases and damage to the bone structures of the pelvis
Brain research
-tumor and inflammatory diseases of the brain;
- malformations of cerebral vessels, intracranial vessels;
- diseases and damage to the bones of the skull and craniovertebral junction;
- acute and chronic cerebrovascular accidents;
- traumatic brain injury of any severity;
-consequences of previous injuries and inflammatory diseases (cysts, hydrocephalus, cortical atrophy)
Spine examination
-degenerative changes (protrusion, herniated intervertebral discs);
- diseases and injuries of the spine (injuries, inflammatory, tumor processes);
-anomalies in the development of spinal structures;
- postoperative changes
Neck examination
- diseases and injuries of the neck organs (larynx, thyroid gland, including tumors, to assess the extent of the process);
- condition of the lymph nodes of the neck;
- diseases and damage to the blood vessels of the neck
Contraindications for CT examination
There are no absolute contraindications for computed tomography.
Contraindications and limitation of indications:
-pregnancy or suspicion of pregnancy
- allergy to iodine-containing drugs during studies with IV contrast with iodine-containing drugs
-menstruation on the day of the study
-reception of barium contrast within the last 10 days
-renal failure
Elements of preparation for RCT examination of the abdominal organs:
- 12 hours fasting break
- 8-12 hours before cleansing enemas to clean water
- after cleansing enemas, drink a diluted solution of 76% urografin or omnipaque 300.350 at the rate of:
Children: 1 ml of contrast per year of life
Adults: dissolve 20 ml (1 ampoule) of contrast in 600 ml of water
- first dose of 2/3 diluted contrast after cleansing enemas 8-12 hours in advance (in the evening before bed, drink within 30-60 minutes)
- second dose of the remaining part of the solution 2 hours before the test (drink within 30 minutes)
Please arrive for the examination 30 minutes in advance.
Have with you: 1 liter of clarified apple juice
List of documents and tests required during hospitalization to conduct an X-ray CT examination under anesthesia:
- referral for RCT examination (+photocopy)
- child's outpatient card
- passport and (or) birth certificate (+photocopies)
- parent's passport (photocopy)
- certificate of exposure to infection (valid for 21 days)
- UAC + leukoformula + coagulability + duration of bleeding (valid 7 days)
- OAM (valid 7 days)
- Pediatrician's report (valid for 7 days)
- ENT doctor's opinion (valid for 7 days)
- feces for eggs\worms, Giardia cysts, scraping for enterobiasis (valid for 7 days)
- children under 2 years old tank. stool culture (valid for 14 days)
12. Mantoux test for all years, polio (vaccination certificate + photocopy)
- for mother, during hospitalization with a child: blood test for RW (valid for 14 days), fluorography with description (valid for 1 year), for mother with children under 2 years old. stool culture is valid for 14 days)
Children are hospitalized for examination under anesthesia the day before! On the day of the examination, do not give the child anything to drink or feed.
Have with you: DVD+RW (for archiving in the department), CD+R (for recording by the patient) if desired,
diaper, shoe covers
It is obligatory to have with you the results of all other studies performed; for repeated CT and MRI examinations, it is obligatory to have with you the results of all previous studies (tomograms, protocols)
List of documents and tests required during hospitalization for RCT examination (without anesthesia)
- referral for research (+photocopies)
- child's outpatient card
- insurance policy, birth certificate and (or) child’s passport (+ photocopies)
4.parent’s passport (+photocopy)
- vaccination certificate (photocopy)
- certificate of contact with infections, pediculosis (valid for 3 days)
- stool test for eggs/worms (valid for 7 days)
- for children over 14 years old: blood test for RW (valid for 14 days, can be done from a finger)
- for children over 15 years of age: blood test for HbsAg and hepatitis C (valid for 1 month), blood test for HIV (valid for 3 months), fluorography (valid for 1 year)
- for a mother during hospitalization with a child: blood test for RW (valid for 14 days), fluorography (valid for 1 year)
Have with you: DVD+RV (for archiving in the department), CD+R (for recording the study for the patient) if desired, a diaper.
Children can be examined without anesthesia within 1 hour. Before the study, in the 8th office of the clinic in the day hospital
It is obligatory to have with you the results of all other studies performed; for repeated CT and MRI examinations, it is obligatory to have with you the results of all previous studies (tomograms, protocols)
List of documents required for RCT examination for outpatients
- referral for research
- patient's outpatient card
- insurance policy, birth certificate and (or) patient’s passport (+ photocopies)
- have with you: DVD+RV (for archiving in the department), CD+R (for recording the study for the patient) if desired, diaper, shoe covers
It is obligatory to have with you the results of all other studies performed; for repeated CT and MRI examinations, it is obligatory to have with you the results of all previous studies (tomograms, protocols)
MRI of a child's brain
The data obtained indicate that more than 70% of the examined patients with ASD had either a history of inflammatory processes, which occurred with complications characteristic of neuroinfection (see Fig. 7), or signs of a chronic inflammatory focus (including on moment of examination) in the structures of the facial skull, anatomically associated with various parts of the brain (see Fig. 1,2), which, apparently, could be the cause of intoxication and allergization of various parts of the central nervous system.
This fact is also confirmed by the fact that 40 patients out of 61 examined showed signs of hypertrophy of the adenoid tonsils, which amounted to 65% of the total number of patients (see Fig. 3)
Also noteworthy is the fact that the ratio of changes detected on MRI is almost equal in the group of patients with childhood and atypical autism (see Diagram 2), which once again indicates the possible trigger role of an infectious-allergic factor in the etiology of the development and course of these forms of autism.
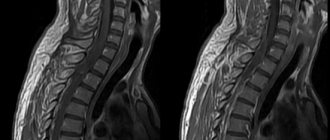
In turn, the presence of changes such as midline cysts and dysgenesis of the corpus callosum (in 37% of cases), related to anomalies in the development of the central nervous system (see Fig. 4, 5, 6), is more indicative of a genetically determined cause of autism .
Conclusions:
From the above it follows:
1. Apparently, against the background of genetic predisposition (taking into account the presence of key phases and stages of the formation of interneuronal connections in the central nervous system), it is the infectious-allergic factor that is the fundamental trigger in the mechanism of occurrence of ASD.
2. MRI examination of the central nervous system should be used as early as possible in all children with central nervous system and, in particular, ASD, not only as the most informative, but also as the most harmless for the purpose of early detection of an infectious-allergic focus that can adversely affect the normal development of the central nervous system and, hence the occurrence of ASD
3. An almost equal ratio of structural changes in the brain and facial skull in childhood and atypical autism may indicate a common etiology and exogenous trigger for these types of ASD.
4. To date, the task remains unsolved, if not eliminating, then at least reducing the toxic effects of anesthesia or sedation on the central nervous system in children with ASD during MRI studies (which is extremely necessary to eliminate motor artifacts that interfere with obtaining a high-quality image).